

Effectiveness of integrase strand transfer inhibitors among treatment-experienced patients in a clinical setting
- PMID: 30870198
- PMCID: PMC6608711
- DOI: 10.1097/QAD.0000000000002194
Effectiveness of integrase strand transfer inhibitors among treatment-experienced patients in a clinical setting
Abstract
Objective: Characterize virologic and immunologic outcomes of INSTI-based antiretroviral therapy (ART) in experienced patients with and without virologic failure.
Design: Prospective clinical cohort.
Methods: ART-experienced, INSTI-naive participants in the University of North Carolina Center for AIDS Research HIV Clinical Cohort (UCHCC) initiating an INSTI-containing regimen 2007-2016 were followed from INSTI initiation (baseline) to the earliest of: outcome of interest, loss to follow-up (LTFU, 1 year without clinical visit), or death. Outcomes of interest were virologic failure (first of two consecutive viral loads at least 200 copies/ml more than 2 weeks apart, or one viral load ≥200 before LTFU) and immune recovery (first CD4 ≥500 cells/μl). Patients with baseline viral load at least 50 copies/ml were given 24 weeks before meeting virologic failure criteria. Kaplan-Meier curves and Cox proportional hazards models compared INSTI regimens and patient characteristics.
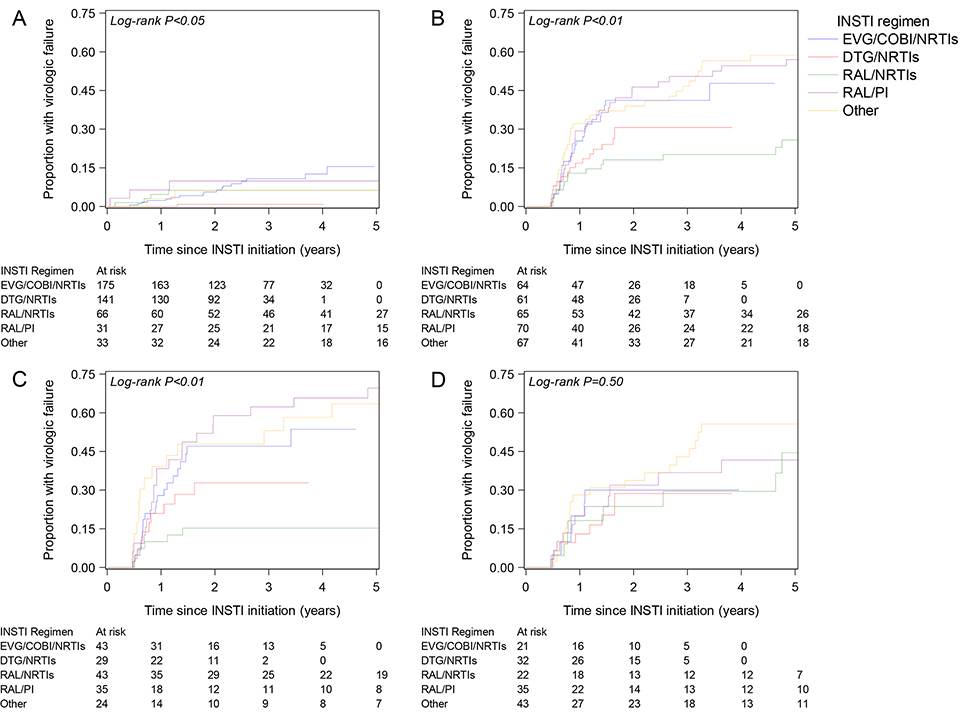
Results: Of 773 patients, 32% were women, 59% African-American, and 42% had a viral load at least 50 copies/ml at INSTI initiation. After 2 years, 5% of patients with baseline viral load less than 50 copies/ml experienced virologic failure, compared with 35% of patients with baseline viral load at least 50 copies/ml (P < 0.01). Among patients with baseline viral load less than 50 copies/ml, dolutegravir/NRTIs was associated with longer time to virologic failure [adjusted hazard ratio (aHR) 0.11, 95% confidence interval (CI) 0.01-0.80], whereas among patients with baseline viral load at least 50 copies/ml, raltegravir/NRTIs was associated with longer time to virologic failure (aHR 0.35, 95% CI 0.18-0.68), both compared with elvitegravir/NRTIs. After 5 years suppressed, irrespective of baseline viral load, 61% of patients experienced immune recovery.
Conclusion: In this cohort, INSTI-containing regimens led to low virologic failure rates in patients switching ART while suppressed. Viremic patients initiating INSTIs were at high risk of virologic failure during follow-up.
Figures
References
-
- Sax PE, DeJesus E, Mills A, et al. Co-formulated elvitegravir, cobicistat, emtricitabine, and tenofovir versus co-formulated efavirenz, emtricitabine, and tenofovir for initial treatment of HIV-1 infection: a randomised, double-blind, phase 3 trial, analysis of results after 48 weeks. Lancet. 2012;379(9835):2439–2448. - PubMed
-
- Walmsley SL, Antela A, Clumeck N, et al. Dolutegravir plus abacavir-lamivudine for the treatment of HIV-1 infection. N Engl J Med. 2013;369(19):1807–1818. - PubMed
-
- Arribas JR, Pialoux G, Gathe J, et al. Simplification to coformulated elvitegravir, cobicistat, emtricitabine, and tenofovir versus continuation of ritonavir-boosted protease inhibitor with emtricitabine and tenofovir in adults with virologically suppressed HIV (STRATEGY-PI): 48 week results of a randomised, open-label, phase 3b, non-inferiority trial. Lancet Infect Dis. 2014;14(7):581–589. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
