

Commensal Candida albicans Positively Calibrates Systemic Th17 Immunological Responses
- PMID: 30870622
- PMCID: PMC6419754
- DOI: 10.1016/j.chom.2019.02.004
Commensal Candida albicans Positively Calibrates Systemic Th17 Immunological Responses
Abstract
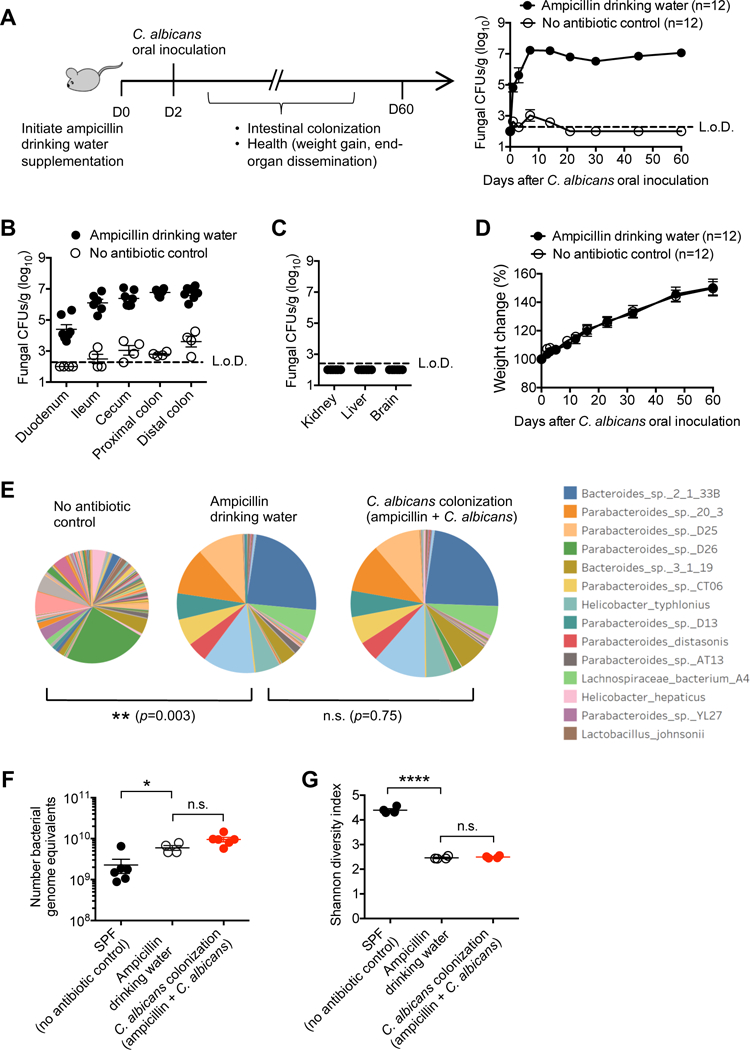
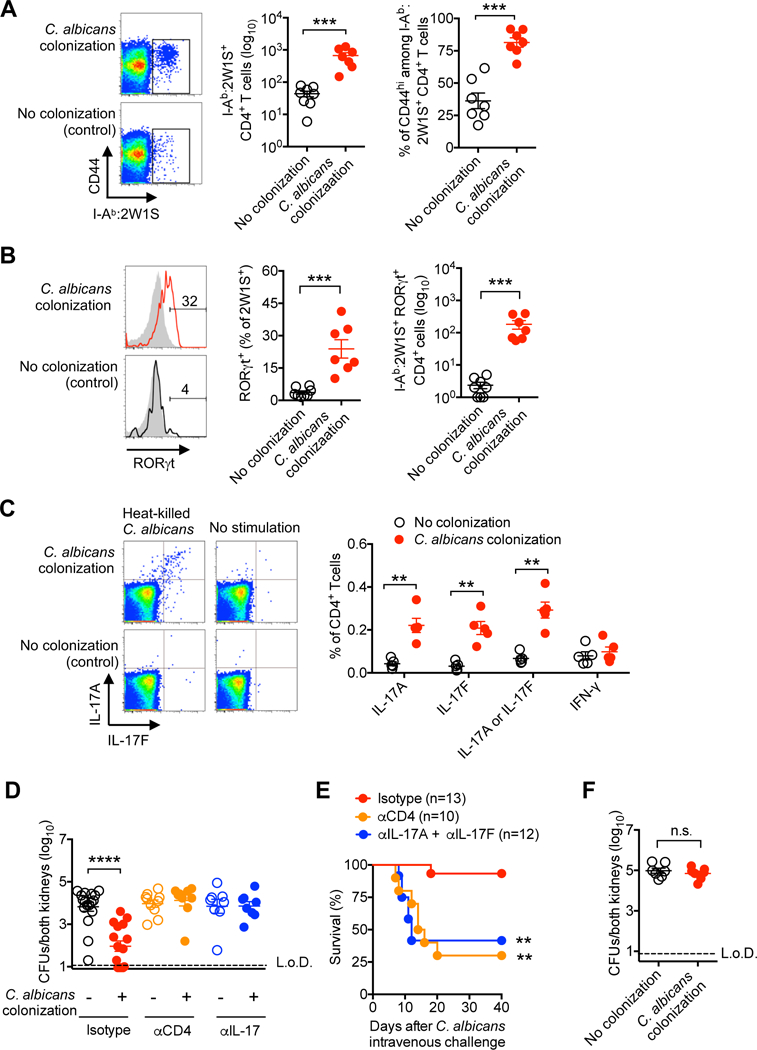
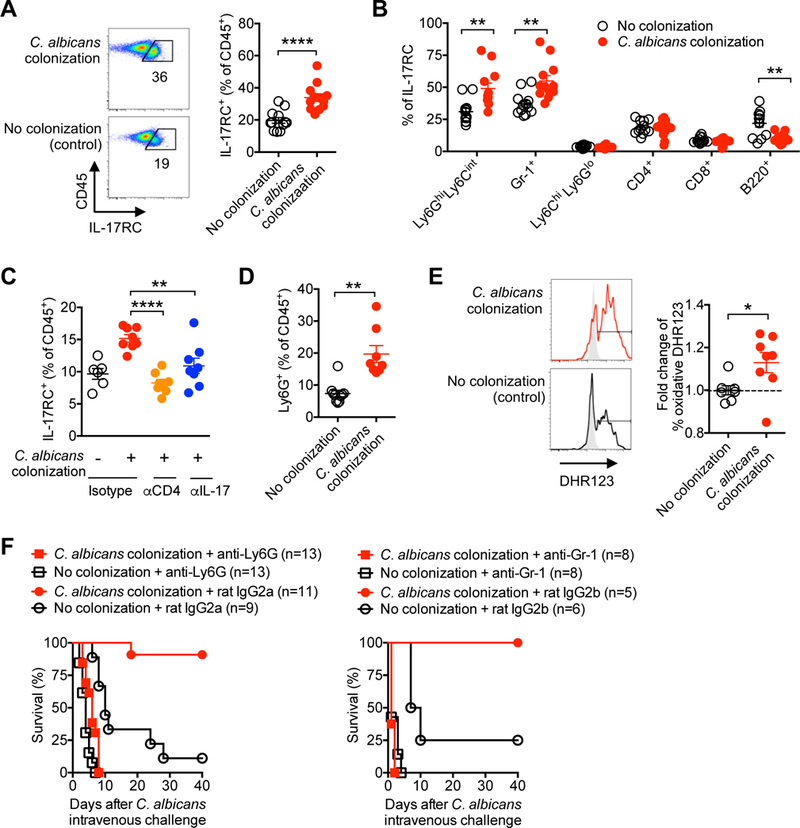
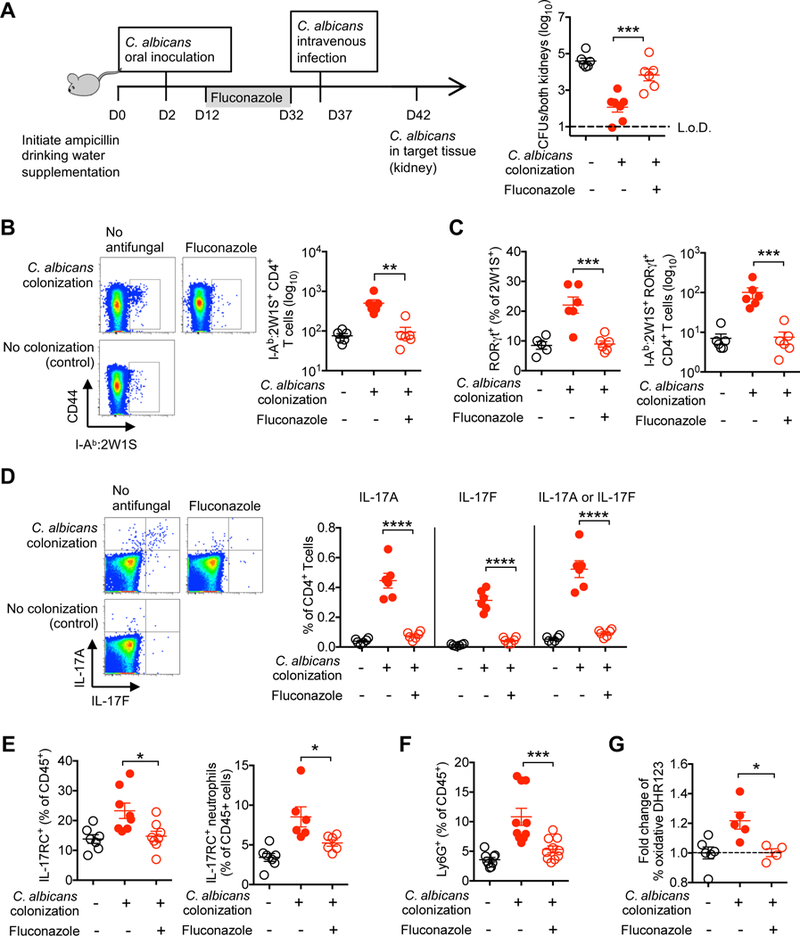
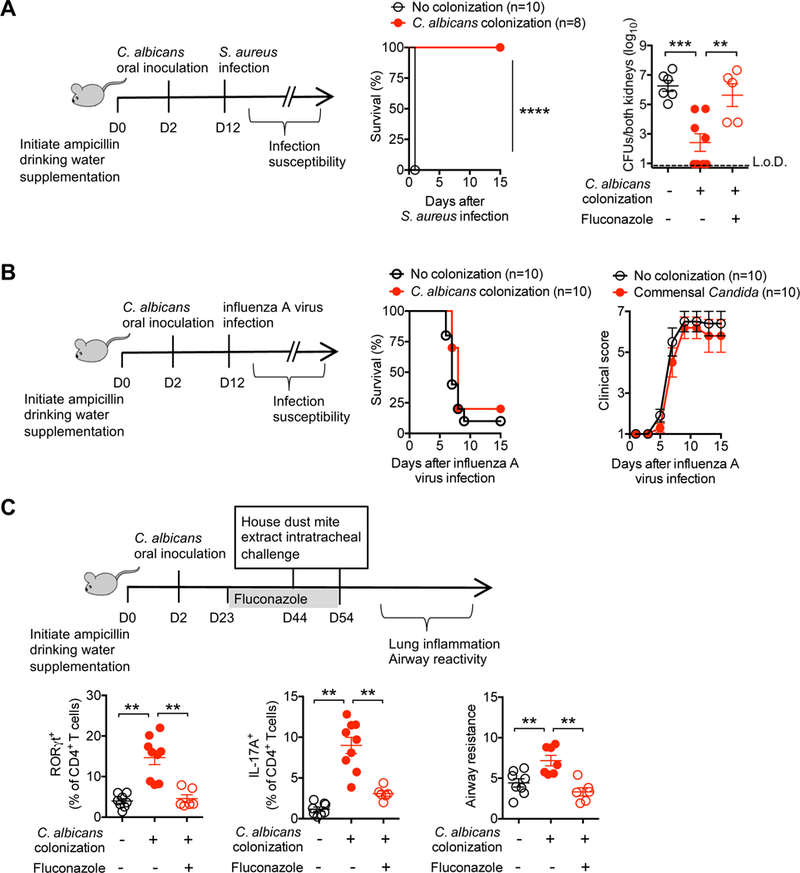
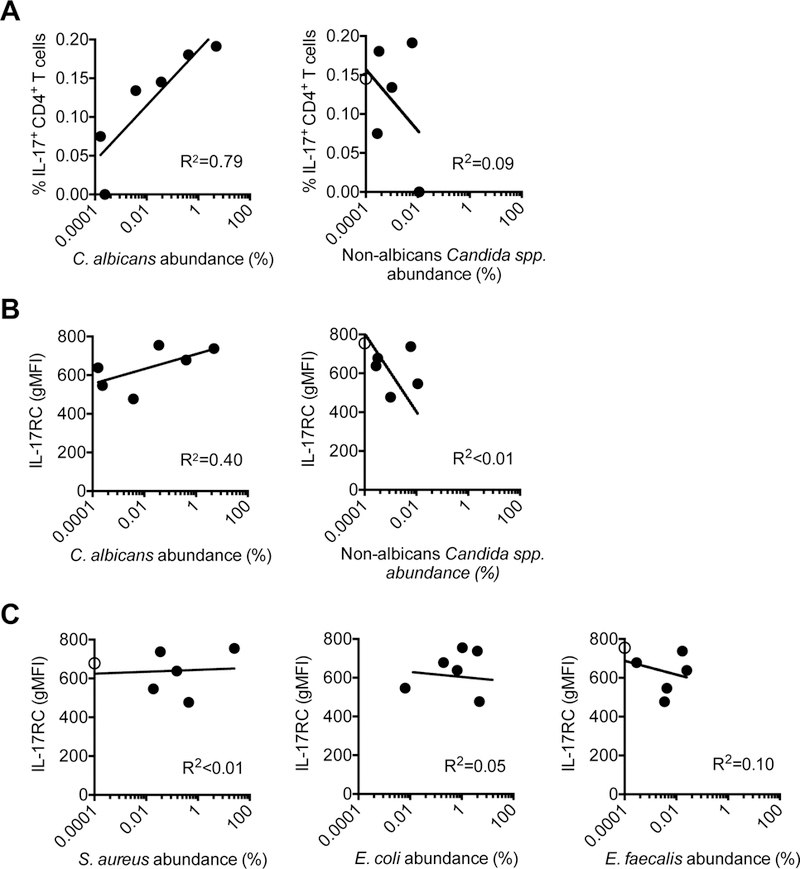
Mucosal barriers are densely colonized by pathobiont microbes such as Candida albicans, capable of invasive disseminated infection. However, systemic infections occur infrequently in healthy individuals, suggesting that pathobiont commensalism may elicit host benefits. We show that intestinal colonization with C. albicans drives systemic expansion of fungal-specific Th17 CD4+ T cells and IL-17 responsiveness by circulating neutrophils, which synergistically protect against C. albicans invasive infection. Protection conferred by commensal C. albicans requires persistent fungal colonization and extends to other extracellular invasive pathogens such as Staphylococcus aureus. However, commensal C. albicans does not protect against intracellular influenza virus infection and exacerbates allergic airway inflammation susceptibility, indicating that positively calibrating systemic Th17 responses is not uniformly beneficial. Thus, systemic Th17 inflammation driven by CD4+ T cells responsive to tonic stimulation by commensal C. albicans improves host defense against extracellular pathogens, but with potentially harmful immunological consequences.
Keywords: CD4 T cells; IL-17; asthma; commensal; fungi; immunity; infection; inflammation; neutrophil; pathobiont.
Copyright © 2019 Elsevier Inc. All rights reserved.
Conflict of interest statement
DECLARATION OF INTERESTS
The authors declare no competing interests.
Figures

References
-
- Acosta-Rodriguez EV, Rivino L, Geginat J, Jarrossay D, Gattorno M, Lanzavecchia A, Sallusto F, and Napolitani G (2007). Surface phenotype and antigenic specificity of human interleukin 17–producing T helper memory cells. Nature immunology 8, 639–646. - PubMed
-
- Acton D, Plat-Sinnige MT, van Wamel W, de Groot N, and van Belkum A (2009). Intestinal carriage of Staphylococcus aureus: how does its frequency compare with that of nasal carriage and what is its clinical impact? European journal of clinical microbiology & infectious diseases 28, 115. - PubMed
-
- Alcorn JF, Crowe CR, and Kolls JK (2010). TH17 cells in asthma and COPD. Annual review of physiology 72, 495–516. - PubMed
-
- Bacher P, Hohnstein T, Beerbaum E, Rocker M, Blango MG, Kaufmann S, Rohmel J, Eschenhagen P, Seidel K, Rickerts V, et al. (2019). Instruction of human anti-fungal Th17 immunity and immune pathology by cross-reactivity against a single member of the microbiota. Cell (in press). - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
