

Association Between Hospital Recognition for Resuscitation Guideline Adherence and Rates of Survival for In-Hospital Cardiac Arrest
- PMID: 30871337
- PMCID: PMC6592630
- DOI: 10.1161/CIRCOUTCOMES.118.005429
Association Between Hospital Recognition for Resuscitation Guideline Adherence and Rates of Survival for In-Hospital Cardiac Arrest
Abstract
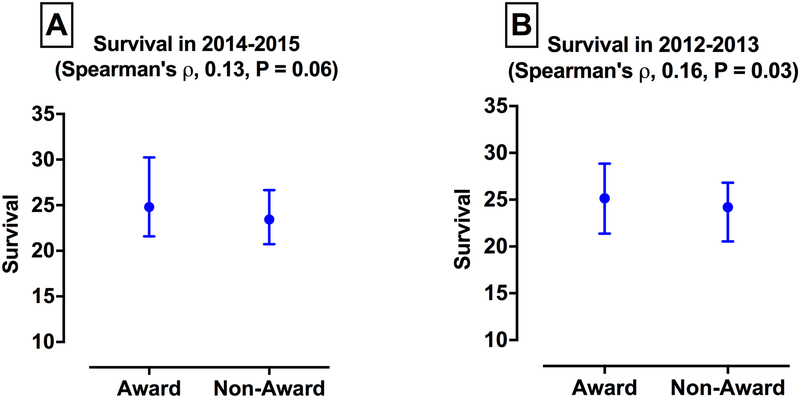
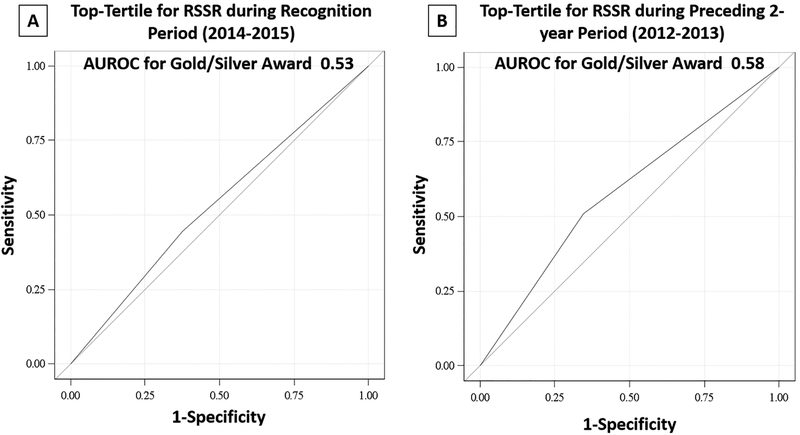
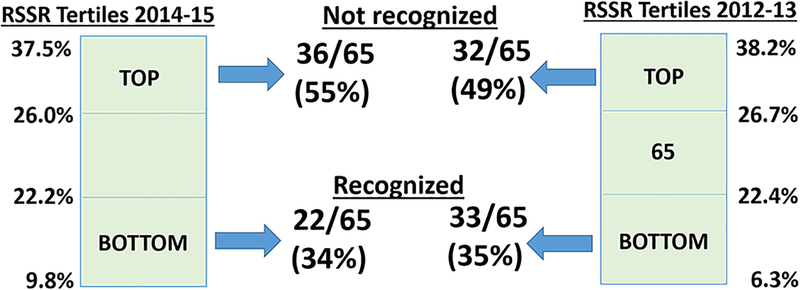
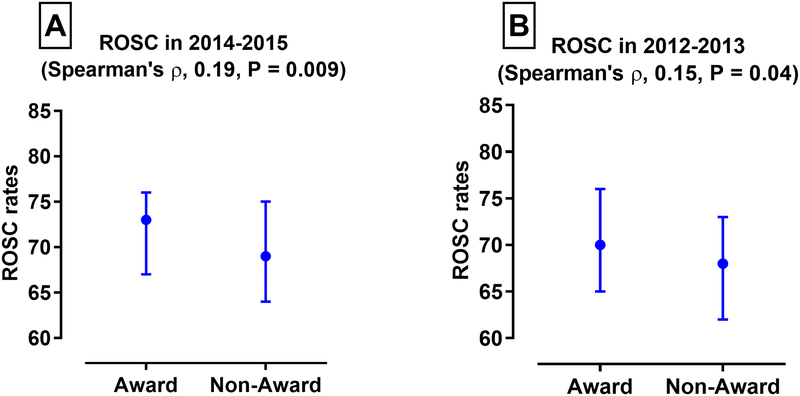
Background Hospitals participating in the national Get With The Guidelines-Resuscitation registry receive an award for high rates of adherence to quality metrics for in-hospital cardiac arrest. We sought to evaluate whether awards based on these quality metrics can be considered a proxy for performance on cardiac arrest survival. Methods and Results Among 195 hospitals with continuous participation in Get With The Guidelines-Resuscitation between 2012 and 2015, we identified 78 that received an award (Gold or Silver) for ≥85% compliance for all 4 metrics for in-hospital cardiac arrest-time to chest compressions, ≤1 minute; time to defibrillation, ≤2 minutes; device confirmation of endotracheal tube placement; and a monitored/witnessed arrest-for at least 12 consecutive months during 2014 to 2015. Award hospitals had higher cardiac arrest volumes than nonaward hospitals but otherwise had similar site characteristics. During 2014 to 2015, award hospitals had higher rates of return of spontaneous circulation for in-hospital cardiac arrest than nonaward hospitals (median [interquartile range], 71% [64%-77%] versus 66% [59%-74%]; Spearman ρ, 0.19; P=0.009). However, rates of risk-standardized survival to discharge at award hospitals (median, 25% [interquartile range, 22%-30%]) were similar to nonaward hospitals (median, 24% [interquartile range, 12%-27%]; Spearman ρ, 0.13; P=0.06). Among hospitals in the best tertile for survival to discharge in 2014 to 2015, 55.4% (36/65) did not receive an award, with poor discrimination of high-performing hospitals by award status (C statistic, 0.53). Similarly, there was only a weak association between hospitals' award status in 2014 to 2015 and their rates of survival to discharge in the preceding 2-year period (Spearman ρ, 0.16; P=0.03). Conclusions The current recognition mechanism within a national registry for in-hospital cardiac arrest captures hospital performance on return of spontaneous circulation but is not well correlated with survival to discharge. This suggests that current awards for resuscitation quality may not adequately capture hospital performance on overall survival-the outcome of greatest interest to patients.
Keywords: heart arrest; outcome and process assessment (health care).
Conflict of interest statement
• Dr. Chan has served as a consultant for the American Heart Association. None of the other authors has any conflicts of interest or financial interests to disclose.
• GWTG-Resuscitation is sponsored by the American Heart Association, which had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication. The manuscript is reviewed and approved by the GWTG-Resuscitation research and publications committee prior to journal submission.
Figures
References
-
- American Heart Association. Get With The Guidelines® - Resuscitation Recognition Criteria. Availble at: https://www.heart.org/en/professional/quality-improvement/get-with-the-g... Accessed December 11, 2018 2016.
-
- Chan PS, Krumholz HM, Nichol G, Nallamothu BK and Investigators AHANRoCR. Delayed time to defibrillation after in-hospital cardiac arrest. N Engl J Med. 2008;358:9–17. - PubMed
-
- Chan PS, Nichol G, Krumholz HM, Spertus JA, Nallamothu BK and Investigators AHANRoCR. Hospital variation in time to defibrillation after in-hospital cardiac arrest. Arch Intern Med. 2009;169:1265–73. - PubMed
-
- Phelan MP, Ornato JP, Peberdy MA, Hustey FM and American Heart Association’s Get With The Guidelines-Resuscitation Investigators. Appropriate documentation of confirmation of endotracheal tube position and relationship to patient outcome from in-hospital cardiac arrest. Resuscitation. 2013;84:31–6. - PubMed
-
- Brady WJ, Gurka KK, Mehring B, Peberdy MA, O’Connor RE and Investigators AHAsGwtG. In-hospital cardiac arrest: impact of monitoring and witnessed event on patient survival and neurologic status at hospital discharge. Resuscitation. 2011;82:845–52. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
