

Guided Self-rehabilitation Contract vs conventional therapy in chronic stroke-induced hemiparesis: NEURORESTORE, a multicenter randomized controlled trial
- PMID: 30871480
- PMCID: PMC6419473
- DOI: 10.1186/s12883-019-1257-y
Guided Self-rehabilitation Contract vs conventional therapy in chronic stroke-induced hemiparesis: NEURORESTORE, a multicenter randomized controlled trial
Abstract
Background: After discharge from hospital following a stroke, prescriptions of community-based rehabilitation are often downgraded to "maintenance" rehabilitation or discontinued. This classic therapeutic behavior stems from persistent confusion between lesion-induced plasticity, which lasts for the first 6 months essentially, and behavior-induced plasticity, of indefinite duration, through which intense rehabilitation might remain effective. This prospective, randomized, multicenter, single-blind study in subjects with chronic stroke-induced hemiparesis evaluates changes in active function with a Guided Self-rehabilitation Contract vs conventional therapy alone, pursued for a year.
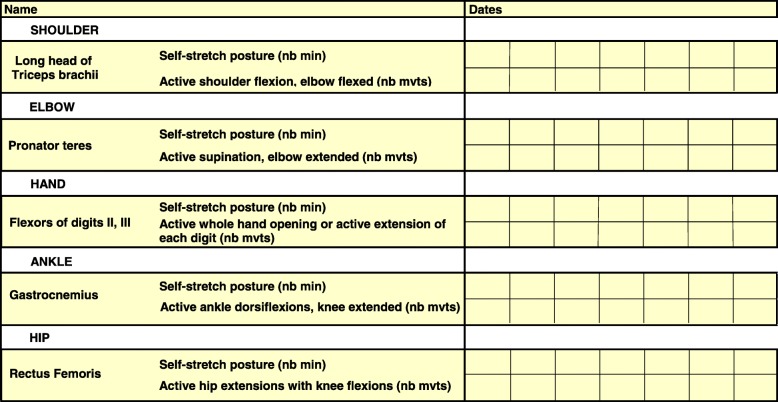
Methods: One hundred and twenty four adult subjects with chronic hemiparesis (> 1 year since first stroke) will be included in six tertiary rehabilitation centers. For each patient, two treatments will be compared over a 1-year period, preceded and followed by an observational 6-month phase of conventional rehabilitation. In the experimental group, the therapist will implement the diary-based and antagonist-targeting Guided Self-rehabilitation Contract method using two monthly home visits. The method involves: i) prescribing a daily antagonist-targeting self-rehabilitation program, ii) teaching the techniques involved in the program, iii) motivating and guiding the patient over time, by requesting a diary of the work achieved to be brought back by the patient at each visit. In the control group, participants will benefit from conventional therapy only, as per their physician's prescription. The two co-primary outcome measures are the maximal ambulation speed barefoot over 10 m for the lower limb, and the Modified Frenchay Scale for the upper limb. Secondary outcome measures include total cost of care from the medical insurance point of view, physiological cost index in the 2-min walking test, quality of life (SF 36) and measures of the psychological impact of the two treatment modalities. Participants will be evaluated every 6 months (D1/M6/M12/M18/M24) by a blinded investigator, the experimental period being between M6 and M18. Each patient will be allowed to receive any medications deemed necessary to their attending physician, including botulinum toxin injections.
Discussion: This study will increase the level of knowledge on the effects of Guided Self-rehabilitation Contracts in patients with chronic stroke-induced hemiparesis.
Trial registration: ClinicalTrials.gov: NCT02202954 , July 29, 2014.
Keywords: Chronic hemiparesis; Motor function; Plasticity; Self-rehabilitation; Stroke.
Conflict of interest statement
Ethics approval and consent to participate
This study is conducted in accordance with the ‘Helsinki Declaration’ and has received ethical approval from “CPP Ile-de-France VI, Groupe Hospitalier Pitié Salpêtrière” (Study Number: P100114 – ID RCB: 2012-A00348–35). Each patient or their legal guardian provided a signed, informed consent to participate to the study. This consent was signed by the patient if possible, or by a third person in the presence of the full conscientious patient. These criteria were approved by the ethics committee.
Consent for publication
Not applicable. This manuscript does not contain an individual person’s data.
Competing interests
JM Gracies served as a consultant for and received research grant support from Allergan, Ipsen, and Merz. The other authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Baer G, Smith M. The recovery of walking ability and subclassification of stroke. Physiother Res Int. 2001;6(3):135–144. - PubMed
-
- Viosca E, Lafuente R, Martínez JL, Almagro PL, Gracia A, González C. Walking recovery after an acute stroke: assessment with a new functional classification and the Barthel index. Arch Phys Med Rehabil. 2005;86(6):1239–1244. - PubMed
-
- Smith MC, Byblow WD, Barber PA, Stinear CM. Proportional recovery from lower limb motor impairment after stroke. Stroke. 2017;48(5):1400–1403. - PubMed
-
- Parker VM, Wade DT, Langton-Hewer R. Loss of arm function after stroke: measurement, frequency and recovery. Internat Rehab Med. 1986;8:69–73. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
