

The oculocardiac reflex and depth of anesthesia measured by brain wave
- PMID: 30871507
- PMCID: PMC6417239
- DOI: 10.1186/s12871-019-0712-z
The oculocardiac reflex and depth of anesthesia measured by brain wave
Abstract
Background: The oculocardiac reflex (OCR), bradycardia that occurs during strabismus surgery is a type of trigemino-cardiac reflex (TCR) is blocked by anticholinergics and enhanced by opioids and dexmedetomidine. Two recent studies suggest that deeper inhalational anesthesia monitored by BIS protects against OCR; we wondered if our data correlated similarly.
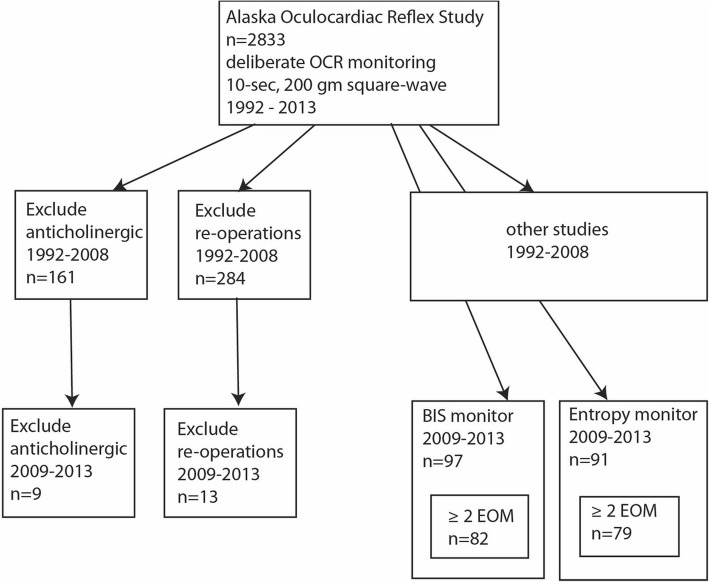
Methods: In an ongoing, prospective study of OCR/TCR elicited by 10-s, 200 g square-wave traction on extraocular muscles (EOM) from 2009 to 2013, anesthetic depth was estimated in cohorts using either BIS or Narcotrend monitors. The depth of anesthesia was deliberately varied between first and second EOM tested.
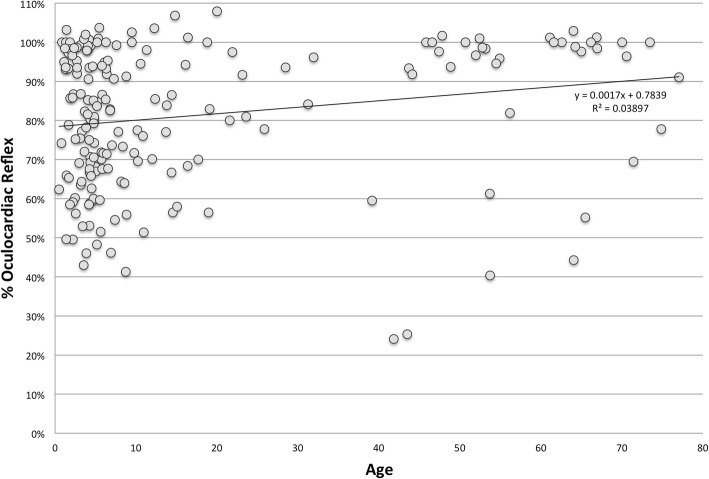
Results: From 1992 through 2013, 2833 cases of OCR during strabismus surgery were monitored. Excluding re-operations and cases with anticholinergic, OCR from first EOM traction averaged - 20.2 ± 21.8% (S.D.) with a range from - 95 to + 25% in patients aged 0.2 to 90 (median 6.5) years. We did not find correlation between %OCR and brain wave for 97 patients with BIS monitoring and 91 with Narcotrend. With intra-patient controls between first and second muscle, the difference in brain wave did not correlate with difference in %OCR for BIS (r = 0.0002, 95% C. I -0.0002, 0.002, p = 0.30) or for Narcotrend (r = - 0.001, 95% C. I -0.004, 0.001, p = 0.32). Secondary multi-variable analysis demonstrated significant association on %OCR particularly with BIS monitor, opioid, propofol and nitrous oxide concentration in the second EOM tensioned. Sevoflurane concentration correlated better with BIS monitor in second and third EOM tension. %OCR correlated with younger age (p < 0.01). OCR with rapid onset was more profound than those with gradual onset (difference in means 18, 95% C. I 10, 26%).
Conclusions: We were unable to confirm a direct correlation between brain wave monitor and OCR when using multifactorial anesthetic agents. The discrepency with other studies probably reflects direct impact of inhalational agent concentration and less deliberate quantification of EOM tension. We found no level of BIS or Entropy EEG monitoring that uniformly prevents OCR.
Trial registry: NCT03663413.
Data: http://www.abcd-vision.org/OCR/OCR%20Brainwave%20de-identified.pdf .
Keywords: Bradycardia; Children; Squint; Trigemino cardiac reflex; Trigeminovagal reflex.
Conflict of interest statement
Authors’ information
MM and LL are pediatric anesthesiologists. ANB is an anesthesiology resident at Wake Forest. RWA is a pediatric ophthalmologists.
Ethics approval and consent to participate
Providence Alaska Medical Center (aka Providence Hospital) (Dr. Judith Whitcomb chair, Initial approval 1992); observational study with consent waived.
Consent for publication
Not applicable.
Competing interests
None with this study.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Schaller B, Cornelius JF, Prabhakar H, Koerbel A, Gnanalingham K, Sandu N, Ottaviani G, Filis A, Buchfelder M. Trigemino-cardiac reflex examination G: the trigemino-cardiac reflex: an update of the current knowledge. J Neurosurg Anesthesiol. 2009;21(3):187–195. doi: 10.1097/ANA.0b013e3181a2bf22. - DOI - PubMed
-
- Machida CJ, Arnold RW. The effect of induced muscle tension and fatigue on the oculocardiac reflex. Binoc Vis and Strabismus Quart. 2003;18(2):81–86. - PubMed
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
