

Pneumonia in severely injured patients with thoracic trauma: results of a retrospective observational multi-centre study
- PMID: 30871601
- PMCID: PMC6419484
- DOI: 10.1186/s13049-019-0608-4
Pneumonia in severely injured patients with thoracic trauma: results of a retrospective observational multi-centre study
Abstract
Background: While the incidence and aspects of pneumonia in ICU patients has been extensively discussed in the literature, studies on the occurrence of pneumonia in severely injured patients are rare. The aim of the present study is to elucidate factors associated with the occurrence of pneumonia in severely injured patients with thoracic trauma.
Setting: Level-I University Trauma Centres associated with the TraumaRegister DGU®.
Methods: A total of 1162 severely injured adult patients with thoracic trauma documented in the TraumaRegister DGU® (TR-DGU) were included in this study. Demographic data, injury severity, duration of mechanical ventilation (MV), duration of ICU stay, occurrence of pneumonia, bronchoalveolar lavage, aspiration, pathogen details, and incidences of mortality were evaluated. Statistical evaluation was performed using SPSS (Version 25.0, SPSS, Inc.) software.
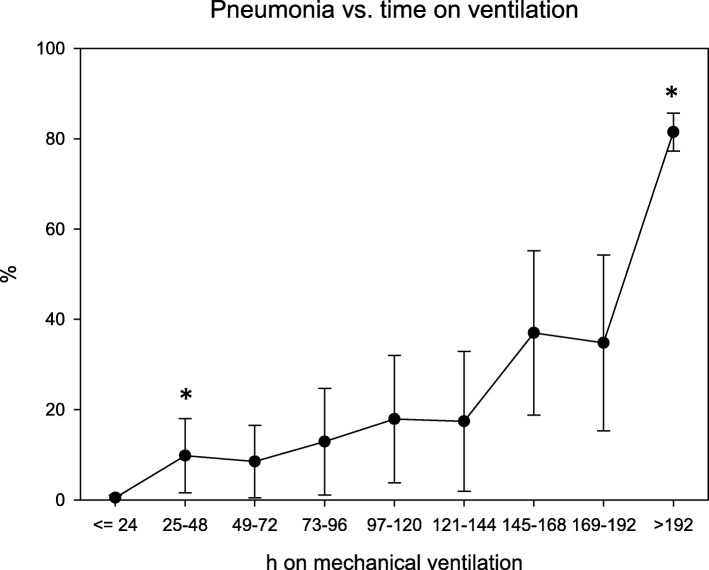
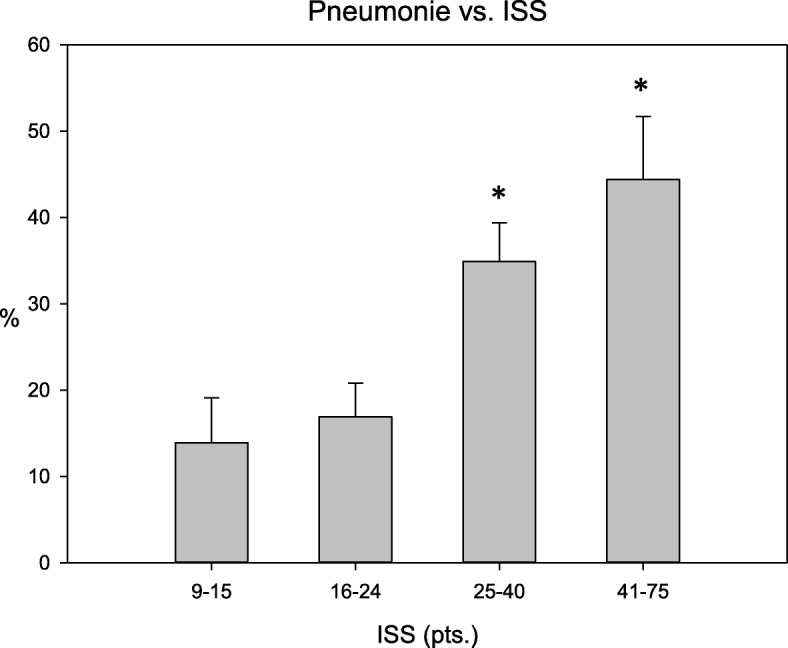
Results: The overall incidence of pneumonia was 27.5%. Compared to patients without pneumonia, patients with pneumonia had sustained more severe injuries (mean ISS: 32.6 vs. 25.4), were older (mean age: 51.3 vs. 47.5) and spent longer periods under MV (mean: 368.9 h vs. 114.9 h). Age, sex (male), aspiration, and duration of MV were all independent predictors for pneumonia occurrence in a multivariate analysis. The cut-off point for duration of MV that best discriminated between patients who would and would not develop pneumonia during their hospital stay was 102 h. The extent of thoracic trauma (AISthorax), ISS, and presence of pulmonary comorbidities did not show significant associations to pneumonia incidence in our multivariate analysis. No significant difference in mortality between patients with and without pneumonia was observed.
Conclusions: Likelihood of pneumonia increases with age, aspiration, and duration of MV. These parameters were not found to be associated with differences in outcomes between patients with and without pneumonia. Future studies should focus on independent parameters to more clearly identify severely injured subgroups with a high risk of developing pneumonia.
Level of evidence: Level II - Retrospective medical record review.
Keywords: AIS; ICU; ISS; Pneumonia; Thoracic trauma.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
The TR-DGU gave permission for publication. All authors read and approved the final manuscript and gave permission for publication.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- DGU®: General annual report 2017. TraumaRegister DGU® 2017.
-
- Batchinsky AI, Weiss WB, Jordan BS, Dick EJ, Jr, Cancelada DA, Cancio LC. Ventilation-perfusion relationships following experimental pulmonary contusion. J Appl Physiol. 2007;103(3):895–902. - PubMed
-
- Huber S, Biberthaler P, Delhey P, Trentzsch H, Winter H, van Griensven M, Lefering R, Huber-Wagner S. Predictors of poor outcomes after significant chest trauma in multiply injured patients: a retrospective analysis from the German Trauma Registry (Trauma Register DGU(R)) Scandinavian journal of trauma, resuscitation and emergency medicine. 2014;22:52. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
