

A Diet Low in Red and Processed Meat Does Not Reduce Rate of Crohn's Disease Flares
- PMID: 30872105
- PMCID: PMC6726378
- DOI: 10.1053/j.gastro.2019.03.015
A Diet Low in Red and Processed Meat Does Not Reduce Rate of Crohn's Disease Flares
Abstract
Background & aims: Diet may be an important factor in the progression of Crohn's disease (CD). We performed a randomized controlled trial to determine whether reduced consumption of red and processed meats decreases the risk of symptomatic relapse of CD, analyzing results from the Food and Crohn's Disease Exacerbation Study (FACES) trial.
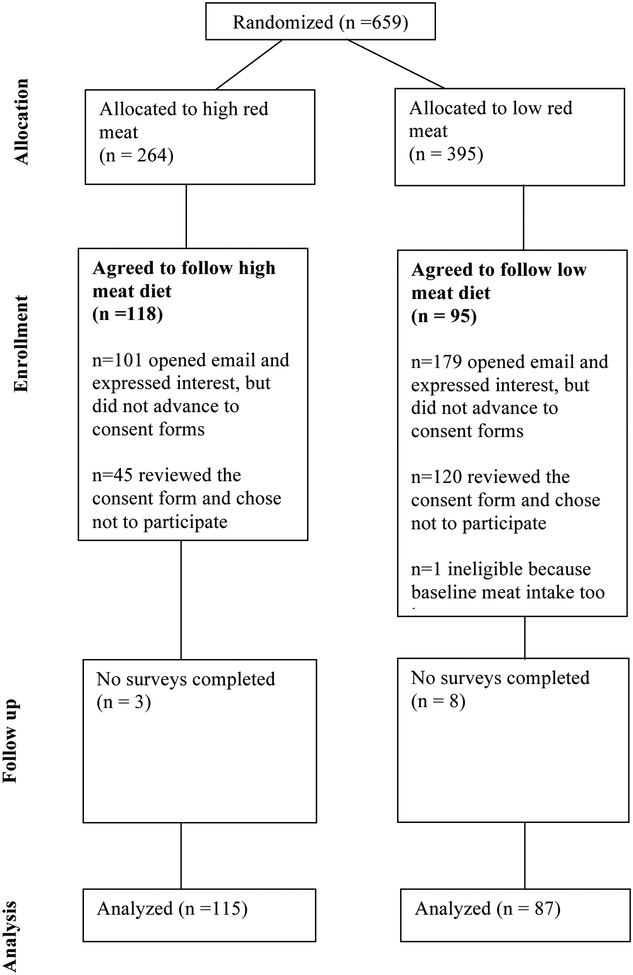
Methods: Adults with CD were recruited into the FACES trial from IBD Partners, an Internet-based cohort of patients with inflammatory bowel disease, from November 2013 through June 2015. Individuals who were in remission (CD activity index [sCDAI] scores of ≤150), had completed a biannual survey, and reported consumption of red meat at least once weekly were randomly assigned to groups that consumed a minimum of 2 servings/week of red or processed meat (high meat, n = 118) or not more than 1 serving per month (low meat, n = 96) for 49 weeks. The primary outcome was relapse of CD, defined as increase in sCDAI score by ≥70 points and to >150 or a need for CD surgery or new CD medication. A secondary outcome, moderate or severe relapse, was based on an increase in sCDAI to >219.
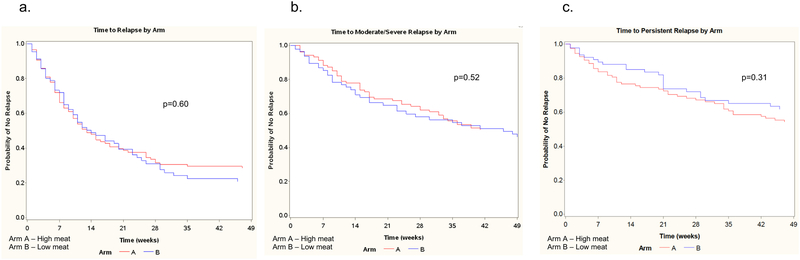
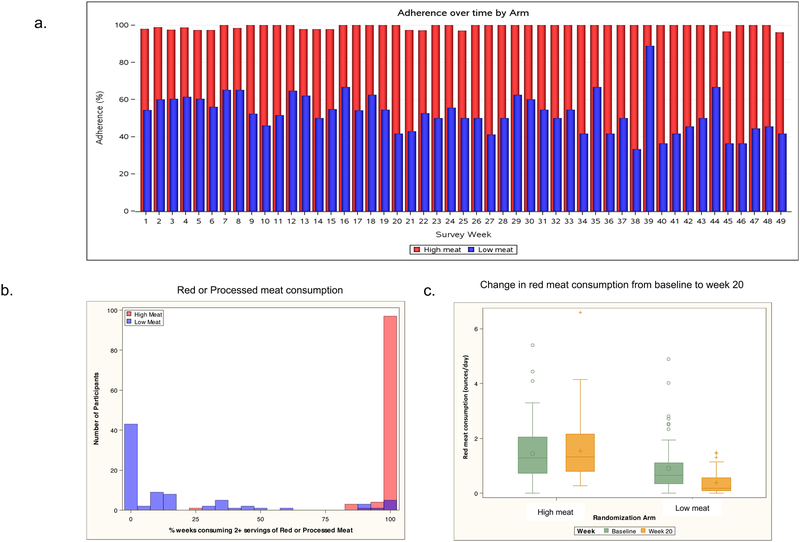
Results: During the trial, the high-meat groups reported consumption of 2 or more servings of red or processed meat during 98.5% of observed weeks compared with 18.8% of weeks for the low-meat group. Any and moderate to severe relapse occurred in 62% of participants in the high-meat group and 42% of participants in the low-meat group. There were no significant differences in time to any (P = .61) or moderate/severe (P = .50) relapse.
Conclusions: In an analysis of data from the FACES trial, we found that among patients with CD in remission, level of red and processed meat consumption was not associated with time to symptomatic relapse. ClinicalTrials.gov, Number: NCT0192673.
Trial registration: ClinicalTrials.gov NCT00192673.
Keywords: IBD; Inflammatory Bowel Disease; Prevention; Quiescent Disease.
Copyright © 2019 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Potential Conflicts of Interest:
Dr. Albenberg has received research funding from Seres Therapeutics.
Dr. Lewis has served as a consultant for: Nestle Health Science, Johnson & Johnson Consumer Inc, Janssen Pharmaceuticals, Takeda, AbbVie, Merck, Celgene, Eli Lilly and Company, Samsung Bioepis, Pfizer, Gilead, UCB, Arena Pharmaceuticals and Bridge Biotherapeutics. He has received research funding from Nestle Health Science, Takeda, and Janssen.
Dr. Kappelman has received research funding from and serves as a consultant for Johnson & Johnson Consumer Inc, Abbvie, Pfizer, and Eli Lilly. He is a shareholder to Johnson & Johnson Consumer Inc.
Figures
References
-
- Lochs H, Dejong C, Hammarqvist F, Hebuterne X, Leon-Sanz M, Schutz T, van Gemert W, van Gossum A, Valentini L, Lubke H, Bischoff S, Engelmann N, Thul P. 2006. ESPEN Guidelines on Enteral Nutrition: Gastroenterology. Clin Nutr 25:260–74. - PubMed
-
- Riordan AM, Hunter JO, Cowan RE, Crampton JR, Davidson AR, Dickinson RJ, Dronfield MW, Fellows IW, Hishon S, Kerrigan GN, et al. 1993. Treatment of active Crohn’s disease by exclusion diet: East Anglian multicentre controlled trial. Lancet 342:1131–4. - PubMed
-
- Bartel G, Weiss I, Turetschek K, Schima W, Puspok A, Waldhoer T, Gasche C. 2008. Ingested matter affects intestinal lesions in Crohn’s disease. Inflamm Bowel Dis 14:374–82. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
