

Neuromyelitis optica spectrum disorders
- PMID: 30872305
- PMCID: PMC6454358
- DOI: 10.7861/clinmedicine.19-2-169
Neuromyelitis optica spectrum disorders
Abstract
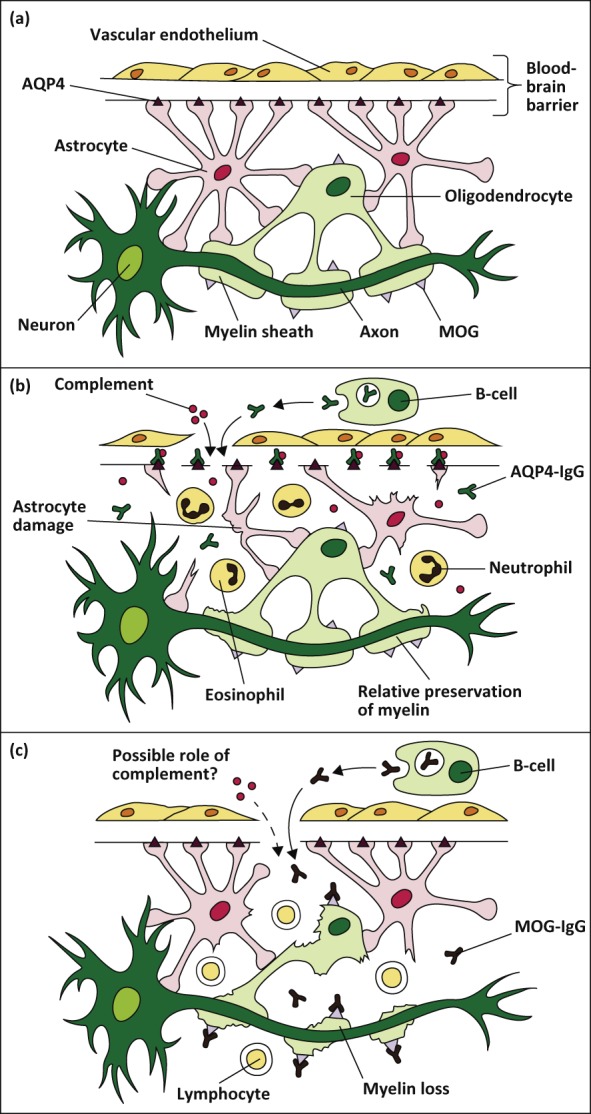
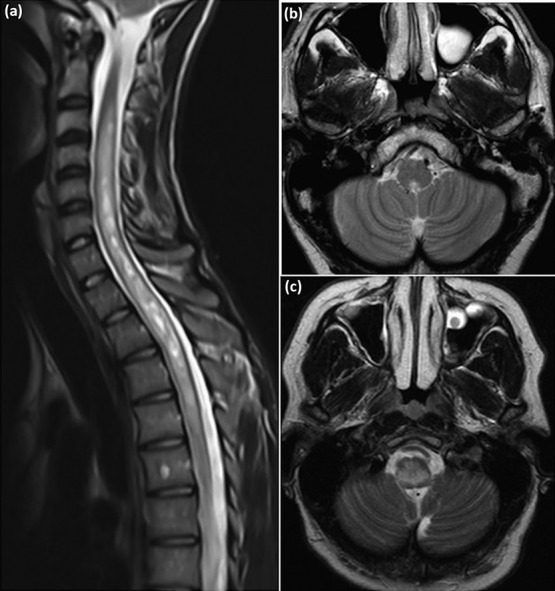
Neuromyelitis optica spectrum disorder (NMOSD) is an uncommon antibody-mediated disease of the central nervous system. Long segments of spinal cord inflammation (myelitis), severe optic neuritis, and/or bouts of intractable vomiting and hiccoughs (area postrema syndrome) are classic presentations of the disease and may alert the clinician to the diagnosis. Untreated, approximately 50% of NMOSD patients will be wheelchair users and blind, and a third will have died within 5 years of their first attack. Unlike multiple sclerosis, a progressive clinical course is very unusual and the accrual of disability is related to relapses. Approximately 75% of patients have antibodies against aquaporin-4, a water channel expressed on astrocytes. Relapses are treated aggressively to prevent residual disability with high-dose steroids and often plasma exchange. Relapse prevention is crucial and achieved with long-term immunosuppression. In this article we review the pathogenesis, clinical features, diagnosis and management of NMOSD.
Keywords: Neuromyelitis optica; antibody; aquaporin-4.
© Royal College of Physicians 2019. All rights reserved.
Figures
References
-
- Lennon VA, Wingerchuk DM, Kryzer TJ, et al. A serum autoantibody marker of neuromyelitis optica: distinction from multiple sclerosis. Lancet 2004;364:2106–12. - PubMed
-
- Kitley J, Woodhall M, Waters P, et al. Myelin-oligodendrocyte glycoprotein antibodies in adults with a neuromyelitis optica phenotype. Neurology 2012;79:1273–7. - PubMed
