

Enrichment of oral microbiota in early cystic precursors to invasive pancreatic cancer
- PMID: 30872392
- PMCID: PMC6872446
- DOI: 10.1136/gutjnl-2018-317458
Enrichment of oral microbiota in early cystic precursors to invasive pancreatic cancer
Abstract
Objectives: Intraductal papillary mucinous neoplasms (IPMNs) are pancreatic cysts that can progress to invasive pancreatic cancer. Associations between oncogenesis and oral microbiome alterations have been reported. This study aims to investigate a potential intracystic pancreatic microbiome in a pancreatic cystic neoplasm (PCN) surgery patient cohort.
Design: Paired cyst fluid and plasma were collected at pancreatic surgery from patients with suspected PCN (n=105). Quantitative and qualitative assessment of bacterial DNA by qPCR, PacBio sequencing (n=35), and interleukin (IL)-1β quantification was performed. The data were correlated to diagnosis, lesion severity and clinical and laboratory profile, including proton-pump inhibitor (PPI) usage and history of invasive endoscopy procedures.
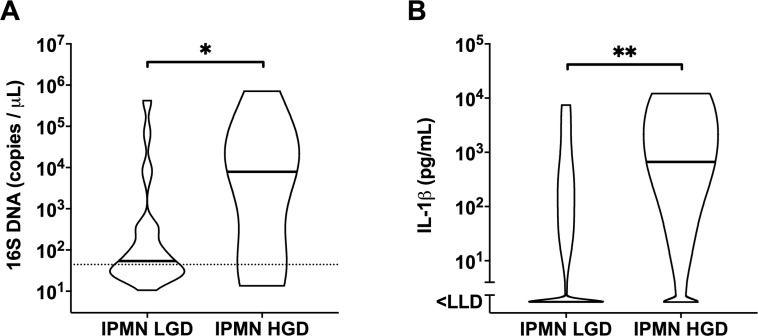
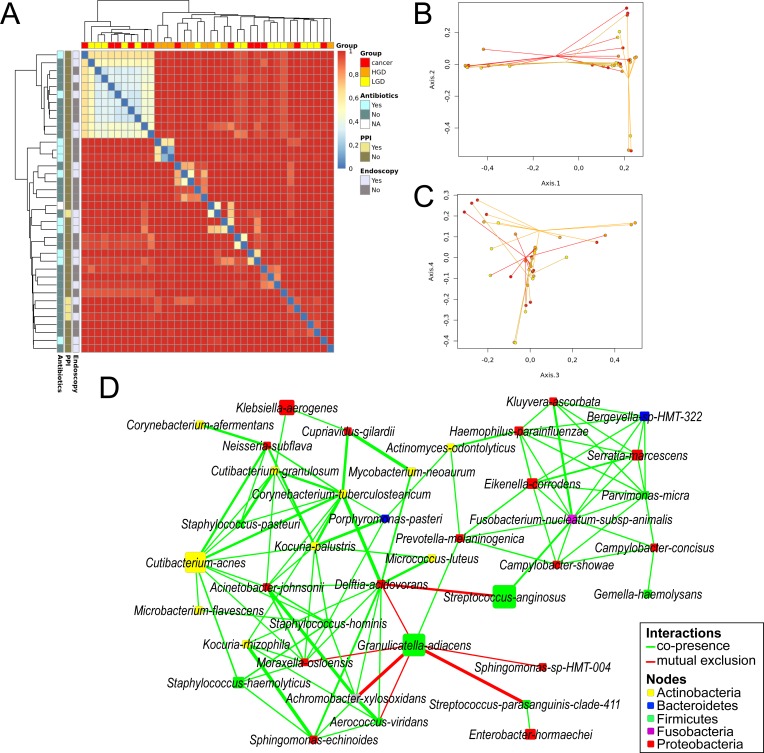
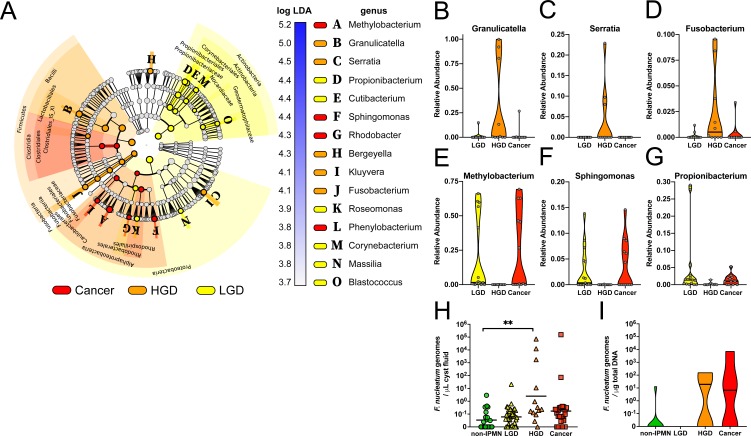
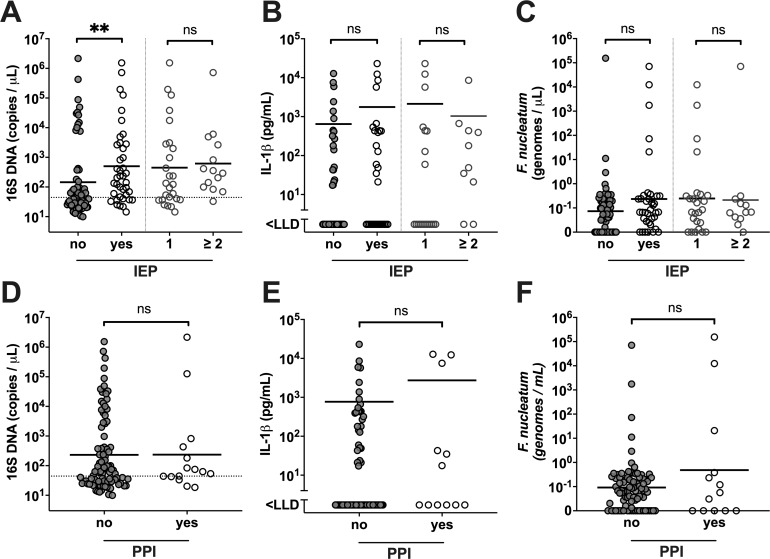
Results: Intracystic bacterial 16S DNA copy number and IL-1β protein quantity were significantly higher in IPMN with high-grade dysplasia and IPMN with cancer compared with non-IPMN PCNs. Despite high interpersonal variation of intracystic microbiota composition, bacterial network and linear discriminant analysis effect size analyses demonstrated co-occurrence and enrichment of oral bacterial taxa including Fusobacterium nucleatum and Granulicatella adiacens in cyst fluid from IPMN with high-grade dysplasia. The elevated intracystic bacterial DNA is associated with, but not limited to, prior exposure to invasive endoscopic procedures, and is independent from use of PPI and antibiotics.
Conclusions: Collectively, these findings warrant further investigation into the role of oral bacteria in cystic precursors to pancreatic cancer and have added values on the aetiopathology as well as the management of pancreatic cysts.
Keywords: bacterial translocation; endoscopic procedure; inflammation; pancreatic surgery; pancreatic tumours.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures


Comment in
-
Tracing the accumulation of in vivo human oral microbiota elucidates microbial community dynamics at the gateway to the GI tract.Gut. 2020 Jul;69(7):1355-1356. doi: 10.1136/gutjnl-2019-318977. Epub 2019 Jun 20. Gut. 2020. PMID: 31227588 Free PMC article. No abstract available.
-
Endoscopic ultrasound (EUS)-guided fine needle biopsy (FNB) formalin fixed paraffin-embedded (FFPE) pancreatic tissue samples are a potential resource for microbiota analysis.Gut. 2021 May;70(5):999-1001. doi: 10.1136/gutjnl-2020-322457. Epub 2020 Aug 18. Gut. 2021. PMID: 32816963 No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases