

Respiratory viral infection: a potential "missing link" in the pathogenesis of COPD
- PMID: 30872396
- PMCID: PMC9488189
- DOI: 10.1183/16000617.0063-2018
Respiratory viral infection: a potential "missing link" in the pathogenesis of COPD
Abstract
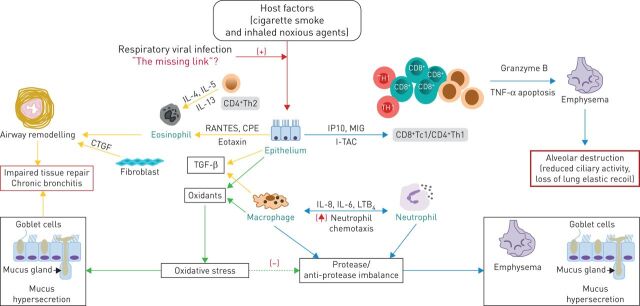
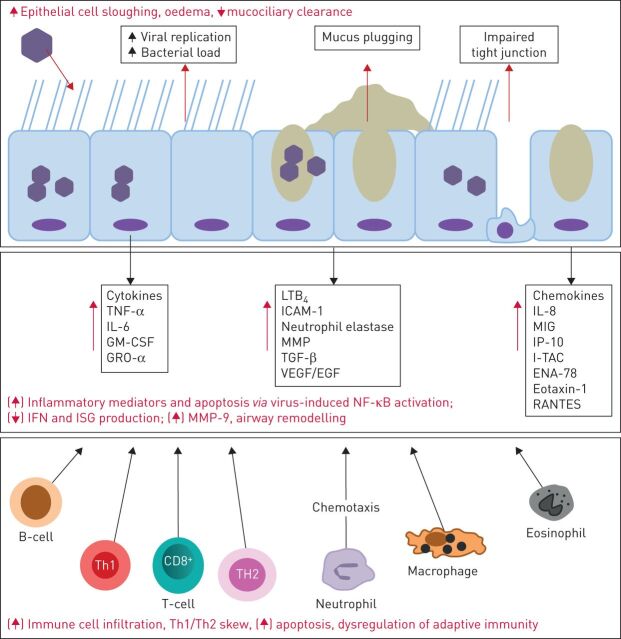
Chronic obstructive pulmonary disease (COPD) is currently the third most common cause of global mortality. Acute exacerbations of COPD frequently necessitate hospital admission to enable more intensive therapy, incurring significant healthcare costs. COPD exacerbations are also associated with accelerated lung function decline and increased risk of mortality. Until recently, bacterial pathogens were believed to be responsible for the majority of disease exacerbations. However, with the advent of culture-independent molecular diagnostic techniques it is now estimated that viruses are detected during half of all COPD exacerbations and are associated with poorer clinical outcomes. Human rhinovirus, respiratory syncytial virus and influenza are the most commonly detected viruses during exacerbation. The role of persistent viral infection (adenovirus) has also been postulated as a potential pathogenic mechanism in COPD. Viral pathogens may play an important role in driving COPD progression by acting as triggers for exacerbation and subsequent lung function decline whilst the role of chronic viral infection remains a plausible hypothesis that requires further evaluation. There are currently no effective antiviral strategies for patients with COPD. Herein, we focus on the current understanding of the cellular and molecular mechanisms of respiratory viral infection in COPD.
Copyright ©ERS 2019.
Conflict of interest statement
Conflict of interest: D. Linden has received grants (salary and research costs) from Mater Hospital YP Trustees. Conflict of interest: H. Guo-Parke has received grants from Pfizer. Conflict of interest: P.V. Coyle has nothing to disclose. Conflict of interest: D. Fairley reports grants to support BHSCT/QUB funding during the conduct of the study, and other support from Hibergene Diagnostics Ltd, outside the submitted work. Conflict of interest: D.F. McAuley has received a grant from the BHSCT YPC Trust, Mater Hospital for to undertake a clinical trial; personal fees (for consultancy) from GlaxoSmithKline, SOBI, Peptinnovate, Boehringer Ingelheim and Bayer; institutional grants from the UK NIHR, Wellcome Trust and other funding from GlaxoSmithKline; and is one of four named inventors on a patent US8962032 covering the use of sialic acid–bearing nanoparticles as anti-inflammatory agents issued to his institution (Queen's University of Belfast). This has no direct impact on the contents of this work. Conflict of interest: C.C. Taggart has received grants from Pfizer UK and other support for consultancy from Albumedix. Conflict of interest: J. Kidney has received grants from Pfizer UK and Mater Hospital YP Trustees. He is also the non-executive director and shareholder of Hibergene Diagnostics Ltd.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical