

Treatment of Idiopathic Achalasia with Per-Oral Esophageal Myotomy
- PMID: 30872910
- PMCID: PMC6411088
- DOI: 10.1016/j.tgie.2018.07.006
Treatment of Idiopathic Achalasia with Per-Oral Esophageal Myotomy
Abstract
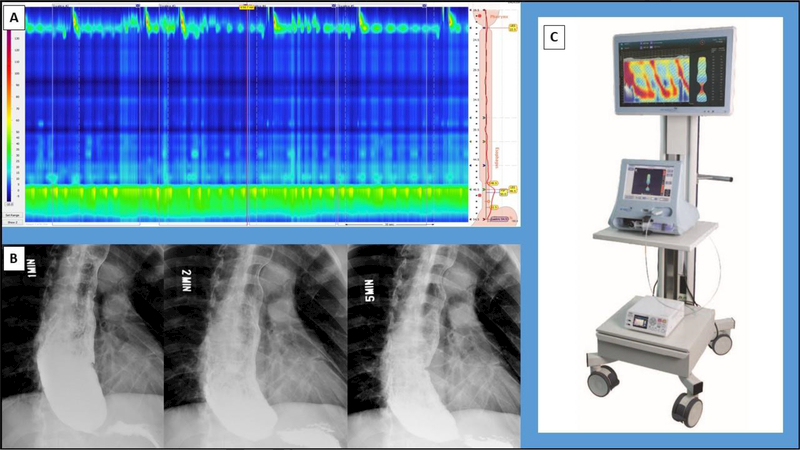
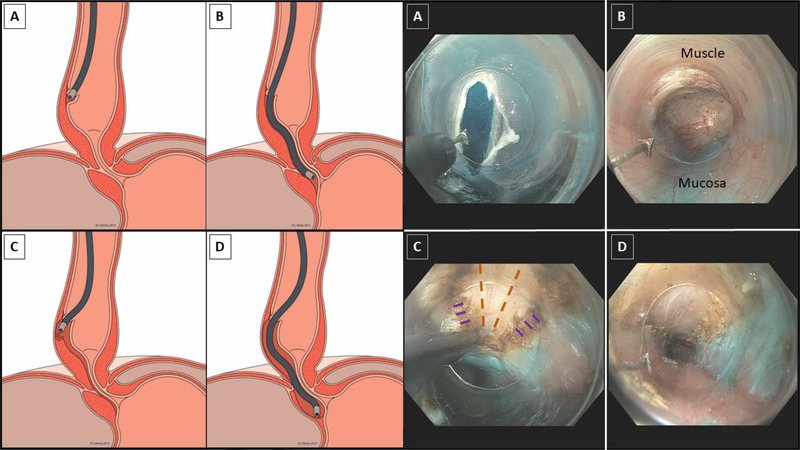
Achalasia is a rare esophageal motility disorder that necessitates the disruption of the lower esophageal sphincter. Patients with achalasia should be evaluated in a systematic, multidisciplinary fashion. Workup should include upper endoscopy, esophagography, and high-resolution manometry. The gold standard for surgical treatment is laparoscopic Heller myotomy with partial fundoplication. Per-oral esophageal myotomy is a novel endoscopic technique that has gained considerable traction over the past decade. The procedure includes the creation of a submucosal tunnel and a selective circular myotomy of the lower esophageal sphincter. Common intra-operative hazards include bleeding within the submucosal tunnel and capnoperitoneum. Significant complications are rare. Patients experience excellent dysphagia relief that is on par with laparoscopic Heller myotomy at moderate-term follow up. Post-operative gastroesophageal reflux disease occurs in greater than one-third of patients, and the vast majority of cases are readily controlled with an anti-secretory medication. Although data is sparse, there is a growing body of literature that supports the long-term durability of per-oral esophageal myotomy.
Keywords: Endoscopic Submucosal Dissection; Endoscopic Surgery; Esophagus; Foregut Surgery; Motility.
Conflict of interest statement
Conflict of Interest Statement: None
Figures
References
-
- Pandolfino JE, Gawron AJ. Achalasia: A systematic review. JAMA 313:1841–1852, 2015 - PubMed
-
- Goldblum JR WR, Orringer MB, Appelman HD. Achalasia. A morphologic study of 42 resected specimens. Am J Surg Pathol 4:327–337, 1994 - PubMed
-
- Boeckxstaens GE, Zaninotto G, Richter JE. Achalasia. The Lancet 383:83–93, 2014 - PubMed
-
- Zaninotto G, Costantini M, Molena D, et al. Minimally Invasive Surgery for Esophageal Achalasia. Journal of Laparoendoscopic & Advanced Surgical Techniques 11:351–359, 2001 - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous