

Pharmacogenetics of FSH Action in the Male
- PMID: 30873114
- PMCID: PMC6403134
- DOI: 10.3389/fendo.2019.00047
Pharmacogenetics of FSH Action in the Male
Abstract
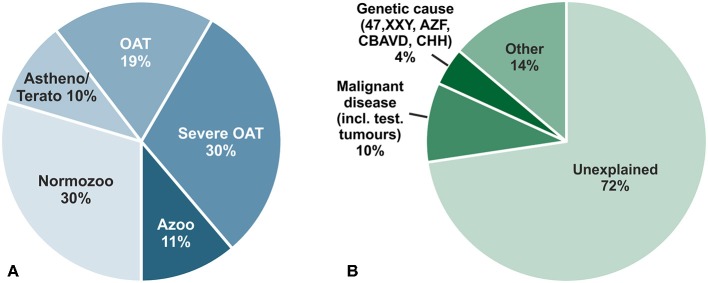
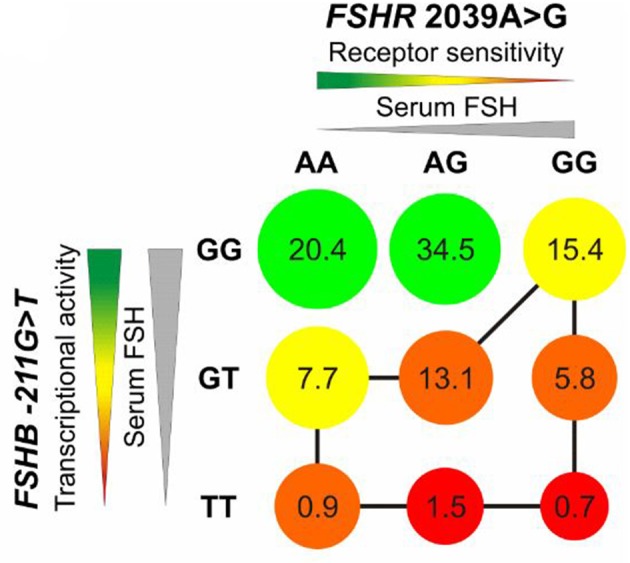
Male infertility is a major contributor to couple infertility, however in most cases it remains "idiopathic" and putative treatment regimens are lacking. This leads to a scenario in which intra-cytoplasmic spermatozoa injection (ICSI) is widely used in idiopathic male infertility, though the treatment burden is high for the couple and it entails considerable costs and risks. Given the crucial role of the Follicle-stimulating hormone (FSH) for spermatogenesis, FSH has been used empirically to improve semen parameters, but the response to FSH varied strongly among treated infertile men. Single nucleotide polymorphisms (SNPs) within FSH ligand/receptor genes (FSHB/FSHR), significantly influencing reproductive parameters in men, represent promising candidates to serve as pharmacogenetic markers to improve prediction of response to FSH. Consequently, several FSH-based pharmacogenetic studies have been conducted within the last years with unfortunately wide divergence concerning selection criteria, treatment and primary endpoints. In this review we therefore outline the current knowledge on single nucleotide polymorphisms (SNPs) in the FSH and FSH receptor genes and their putative functional effects. We compile and critically assess the previously performed pharmacogenetic studies in the male and propose a putative strategy that might allow identifying patients who could benefit from FSH treatment.
Keywords: FSH; genetics; idiopathic male infertility; pharmacogenetic studies; single nucleotide polymorphism (SNP); spermatogenesis.
Figures


Similar articles
-
FSHB -211G>T stratification for follicle-stimulating hormone treatment of male infertility patients: making the case for a pharmacogenetic approach in genetic functional secondary hypogonadism.Andrology. 2015 Nov;3(6):1050-3. doi: 10.1111/andr.12094. Epub 2015 Oct 7. Andrology. 2015. PMID: 26445243
-
Treatment with human, recombinant FSH improves sperm DNA fragmentation in idiopathic infertile men depending on the FSH receptor polymorphism p.N680S: a pharmacogenetic study.Hum Reprod. 2016 Sep;31(9):1960-9. doi: 10.1093/humrep/dew167. Epub 2016 Jun 20. Hum Reprod. 2016. PMID: 27329968 Clinical Trial.
-
FSHB -211 G>T is a major genetic modulator of reproductive physiology and health in childbearing age women.Hum Reprod. 2018 May 1;33(5):954-966. doi: 10.1093/humrep/dey057. Hum Reprod. 2018. PMID: 29617818
-
Mechanisms in endocrinology: Genetics of FSH action: a 2014-and-beyond view.Eur J Endocrinol. 2014 Feb 4;170(3):R91-107. doi: 10.1530/EJE-13-0624. Print 2014 Mar. Eur J Endocrinol. 2014. PMID: 24288354 Review.
-
Pharmacogenetics of follicle-stimulating hormone action in the male.Andrology. 2025 Apr 30. doi: 10.1111/andr.70053. Online ahead of print. Andrology. 2025. PMID: 40304702 Review.
Cited by
-
Development of a novel next-generation sequencing panel for diagnosis of quantitative spermatogenic impairment.J Assist Reprod Genet. 2020 Apr;37(4):753-762. doi: 10.1007/s10815-020-01747-0. Epub 2020 Apr 3. J Assist Reprod Genet. 2020. PMID: 32242295 Free PMC article.
-
Advances in the Regulation of Mammalian Follicle-Stimulating Hormone Secretion.Animals (Basel). 2021 Apr 15;11(4):1134. doi: 10.3390/ani11041134. Animals (Basel). 2021. PMID: 33921032 Free PMC article. Review.
-
An overview of FSH-FSHR biology and explaining the existing conundrums.J Ovarian Res. 2021 Oct 30;14(1):144. doi: 10.1186/s13048-021-00880-3. J Ovarian Res. 2021. PMID: 34717708 Free PMC article. Review.
-
Identification of deleterious variants associated with male infertility genes in a cohort of idiopathic hypospermatogenesis patients.Front Reprod Health. 2025 Jan 3;6:1494585. doi: 10.3389/frph.2024.1494585. eCollection 2024. Front Reprod Health. 2025. PMID: 39830005 Free PMC article.
-
Changes in pituitary gonadotropin subunits and hypothalamic Kiss-1 gene expression by administration of sex steroids in ovary-intact female rats.Endocrine. 2024 Mar;83(3):733-746. doi: 10.1007/s12020-023-03596-0. Epub 2023 Nov 15. Endocrine. 2024. PMID: 37966704
References
-
- Jungwirth A, Diemer T, Dohle GR, Giwercman A, Kopa Z, Krausz C, et al. Guidelines on male infertility. In: European Association of Urology (2015). p. 1–42. Available online at: https://uroweb.org/wp-content/uploads/17-Male-Infertility_LR1.pdf
-
- Busch AS, Kliesch S, Tüttelmann F, Gromoll J. FSHB−211G>T stratification for follicle-stimulating hormone treatment of male infertility patients: making the case for a pharmacogenetic approach in genetic functional secondary hypogonadism. Andrology. (2015) 3:1050–3. 10.1111/andr.12094 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources