

Angioplasty in asymptomatic carotid artery stenosis vs. endarterectomy compared to best medical treatment: One-year interim results of SPACE-2
- PMID: 30873912
- PMCID: PMC7416333
- DOI: 10.1177/1747493019833017
Angioplasty in asymptomatic carotid artery stenosis vs. endarterectomy compared to best medical treatment: One-year interim results of SPACE-2
Abstract
Background: Treatment of individuals with asymptomatic carotid artery stenosis is still handled controversially. Recommendations for treatment of asymptomatic carotid stenosis with carotid endarterectomy (CEA) are based on trials having recruited patients more than 15 years ago. Registry data indicate that advances in best medical treatment (BMT) may lead to a markedly decreasing risk of stroke in asymptomatic carotid stenosis. The aim of the SPACE-2 trial (ISRCTN78592017) was to compare the stroke preventive effects of BMT alone with that of BMT in combination with CEA or carotid artery stenting (CAS), respectively, in patients with asymptomatic carotid artery stenosis of ≥70% European Carotid Surgery Trial (ECST) criteria.
Methods: SPACE-2 is a randomized, controlled, multicenter, open study. A major secondary endpoint was the cumulative rate of any stroke (ischemic or hemorrhagic) or death from any cause within 30 days plus an ipsilateral ischemic stroke within one year of follow-up. Safety was assessed as the rate of any stroke and death from any cause within 30 days after CEA or CAS. Protocol changes had to be implemented. The results on the one-year period after treatment are reported.
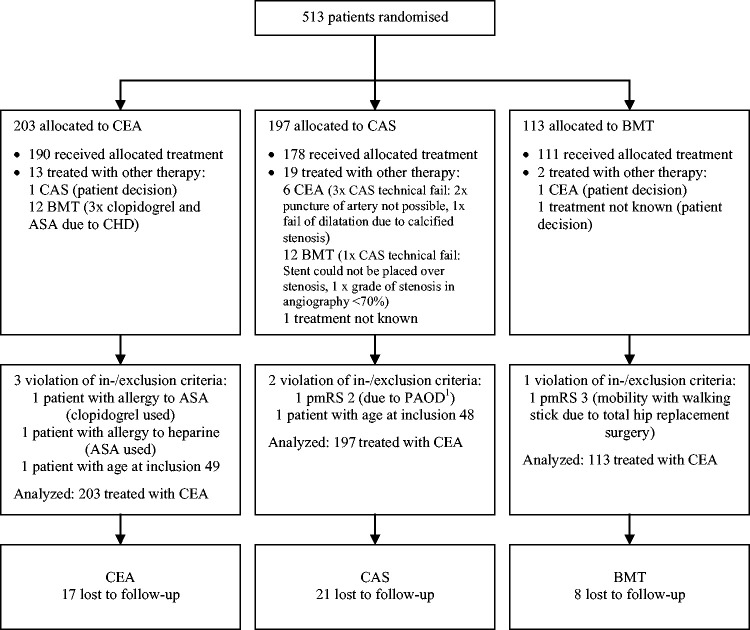
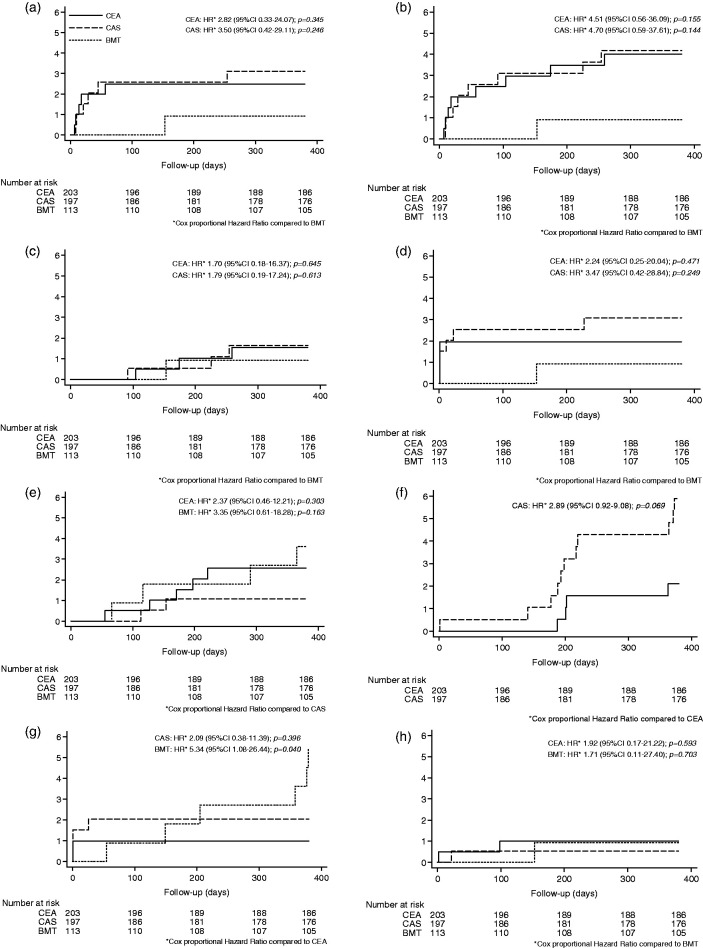
Findings: It was planned to enroll 3550 patients. Due to low recruitment, the enrollment of patients was stopped prematurely after randomization of 513 patients in 36 centers to CEA (n = 203), CAS (n = 197), or BMT (n = 113). The one-year rate of the major secondary endpoint did not significantly differ between groups (CEA 2.5%, CAS 3.0%, BMT 0.9%; p = 0.530) as well as rates of any stroke (CEA 3.9%, CAS 4.1%, BMT 0.9%; p = 0.256) and all-cause mortality (CEA 2.5%, CAS 1.0%, BMT 3.5%; p = 0.304). About half of all strokes occurred in the peri-interventional period. Higher albeit statistically non-significant rates of restenosis occurred in the stenting group (CEA 2.0% vs. CAS 5.6%; p = 0.068) without evidence of increased stroke rates.
Interpretation: The low sample size of this prematurely stopped trial of 513 patients implies that its power is not sufficient to show that CEA or CAS is superior to a modern medical therapy (BMT) in the primary prevention of ischemic stroke in patients with an asymptomatic carotid stenosis up to one year after treatment. Also, no evidence for differences in safety between CAS and CEA during the first year after treatment could be derived. Follow-up will be performed up to five years. Data may be used for pooled analysis with ongoing trials.
Keywords: Asymptomatic carotid artery stenosis; best medical treatment; carotid artery stenting; carotid endarterectomy; disease-free survival; epidemiology; primary prevention; prospective study; stroke.
Figures
References
-
- de Weerd M, Greving JP, de Jong AW, Buskens E, Bots ML. Prevalence of asymptomatic carotid artery stenosis according to age and sex: systematic review and metaregression analysis. Stroke 2009; 40: 1105–1113. - PubMed
-
- Venermo M, Wang G, Sedrakyan A, et al. Editor's choice – carotid stenosis treatment: variation in international practice patterns. Eur J Vasc Endovasc Surg 2017; 53: 511–519. - PubMed
-
- Schneider PA, Naylor AR. Asymptomatic carotid artery stenosis – medical therapy alone versus medical therapy plus carotid endarterectomy or stenting. J Vasc Surg 2010; 52: 499–507. - PubMed
