

Copy number alterations in B-cell development genes, drug resistance, and clinical outcome in pediatric B-cell precursor acute lymphoblastic leukemia
- PMID: 30874617
- PMCID: PMC6420659
- DOI: 10.1038/s41598-019-41078-4
Copy number alterations in B-cell development genes, drug resistance, and clinical outcome in pediatric B-cell precursor acute lymphoblastic leukemia
Abstract
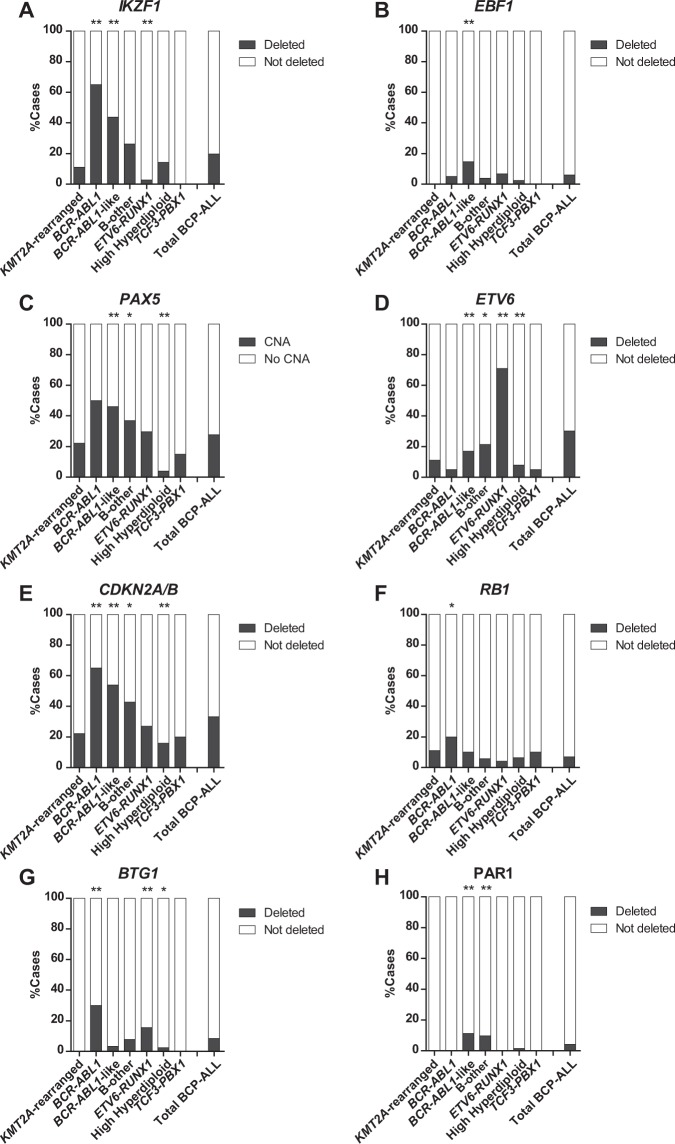
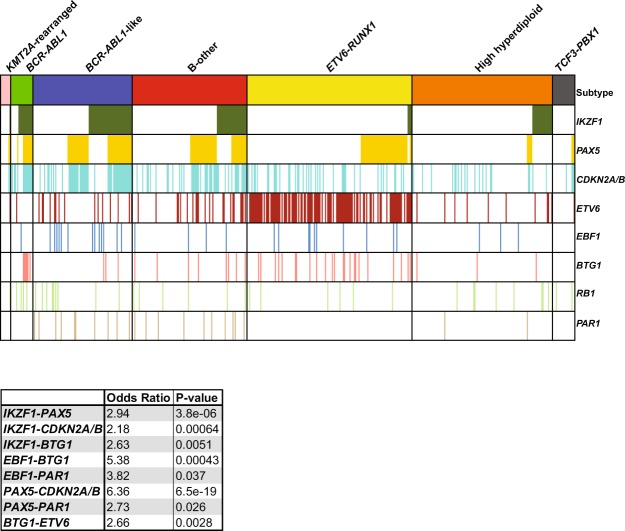
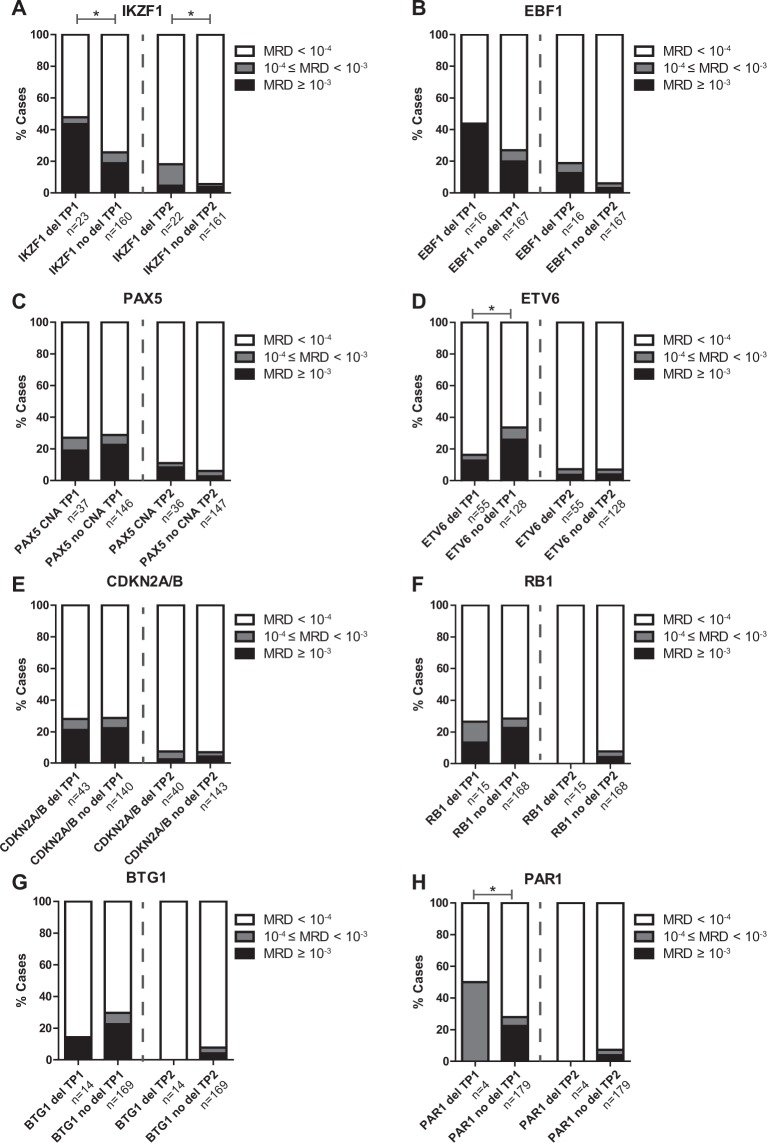
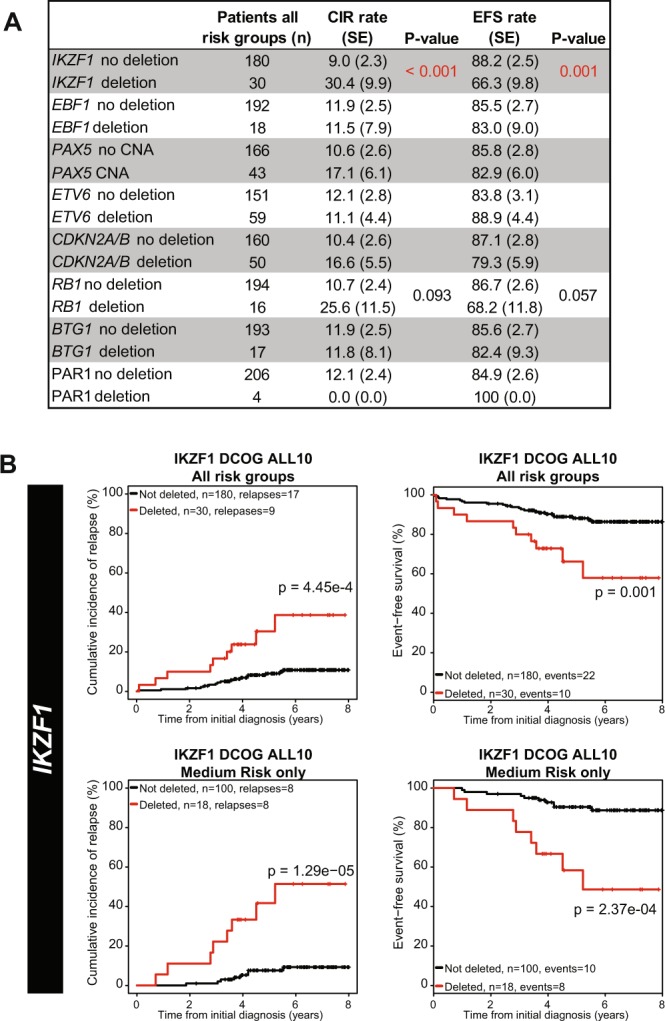
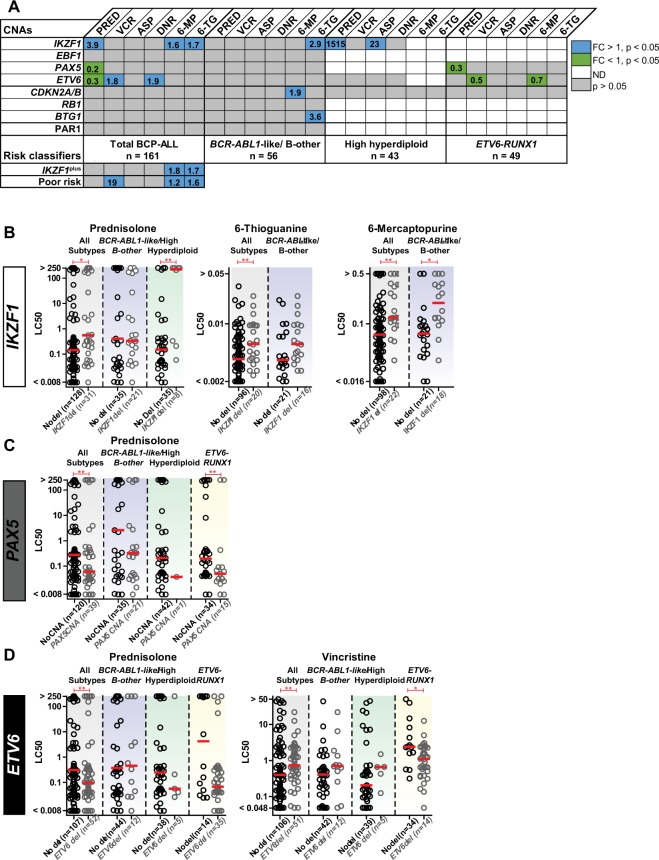
Pediatric B-cell precursor acute lymphoblastic leukemia (BCP-ALL) is associated with a high frequency of copy number alterations (CNAs) in IKZF1, EBF1, PAX5, CDKN2A/B, RB1, BTG1, ETV6, and/or the PAR1 region (henceforth: B-cell development genes). We aimed to gain insight in the association between CNAs in these genes, clinical outcome parameters, and cellular drug resistance. 71% of newly diagnosed pediatric BCP-ALL cases harbored one or more CNAs in these B-cell development genes. The distribution and clinical relevance of these CNAs was highly subtype-dependent. In the DCOG-ALL10 cohort, only loss of IKZF1 associated as single marker with unfavorable outcome parameters and cellular drug resistance. Prednisolone resistance was observed in IKZF1-deleted primary high hyperdiploid cells (~1500-fold), while thiopurine resistance was detected in IKZF1-deleted primary BCR-ABL1-like and non-BCR-ABL1-like B-other cells (~2.7-fold). The previously described risk stratification classifiers, i.e. IKZF1plus and integrated cytogenetic and CNA classification, both predicted unfavorable outcome in the DCOG-ALL10 cohort, and associated with ex vivo drug cellular resistance to thiopurines, or L-asparaginase and thiopurines, respectively. This resistance could be attributed to overrepresentation of BCR-ABL1-like cases in these risk groups. Taken together, our data indicate that the prognostic value of CNAs in B-cell development genes is linked to subtype-related drug responses.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Pieters R, et al. Successful Therapy Reduction and Intensification for Childhood Acute Lymphoblastic Leukemia Based on Minimal Residual Disease Monitoring: Study ALL10 From the Dutch Childhood Oncology Group. Journal of clinical oncology: official journal of the American Society of Clinical Oncology. 2016;34:2591–2601. doi: 10.1200/JCO.2015.64.6364. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
