

Effect of Catheter Ablation vs Medical Therapy on Quality of Life Among Patients With Atrial Fibrillation: The CABANA Randomized Clinical Trial
- PMID: 30874716
- PMCID: PMC6450275
- DOI: 10.1001/jama.2019.0692
Effect of Catheter Ablation vs Medical Therapy on Quality of Life Among Patients With Atrial Fibrillation: The CABANA Randomized Clinical Trial
Erratum in
-
Error in the Results.JAMA. 2019 Jun 18;321(23):2370. doi: 10.1001/jama.2019.7682. JAMA. 2019. PMID: 31211327 Free PMC article. No abstract available.
Abstract
Importance: Catheter ablation is more effective than drug therapy in restoring sinus rhythm in patients with atrial fibrillation (AF), but its incremental effect on long-term quality of life (QOL) is uncertain.
Objective: To determine whether catheter ablation is more beneficial than conventional drug therapy for improving QOL in patients with AF.
Design, setting, and participants: An open-label randomized clinical trial of catheter ablation vs drug therapy in 2204 symptomatic patients with AF older than 65 years or 65 years or younger with at least 1 risk factor for stroke. Patients were enrolled from November 2009 to April 2016 from 126 centers in 10 countries. Follow-up ended in December 2017.
Interventions: Pulmonary vein isolation, with additional ablation procedures at the discretion of the investigators, for the catheter ablation group (n = 1108) and standard rhythm and/or rate-control drugs selected and managed by investigators for the drug therapy group (n = 1096).
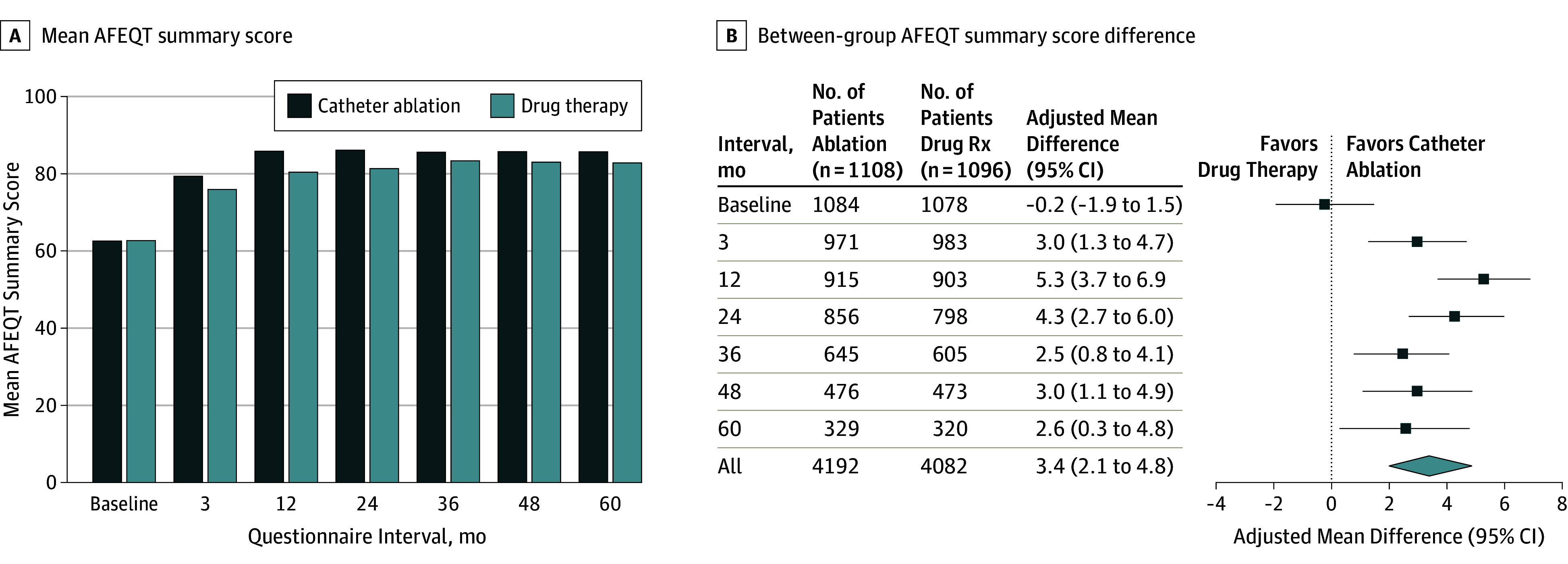
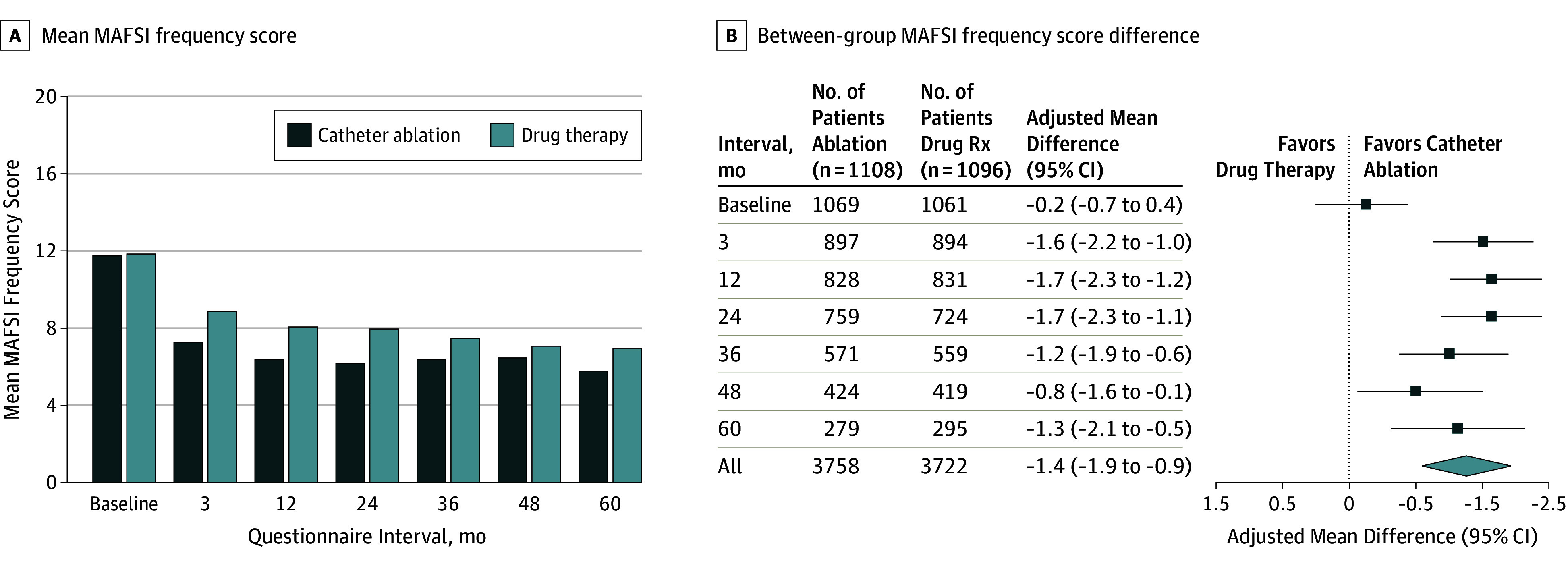
Main outcomes and measures: Prespecified co-primary QOL end points at 12 months, including the Atrial Fibrillation Effect on Quality of Life (AFEQT) summary score (range, 0-100; 0 indicates complete disability and 100 indicates no disability; patient-level clinically important difference, ≥5 points) and the Mayo AF-Specific Symptom Inventory (MAFSI) frequency score (range, 0-40; 0 indicates no symptoms and 40 indicates the most severe symptoms; patient-level clinically important difference, ≤-1.6 points) and severity score (range, 0-30; 0 indicates no symptoms and 30 indicates the most severe symptoms; patient-level clinically important difference, ≤-1.3 points).
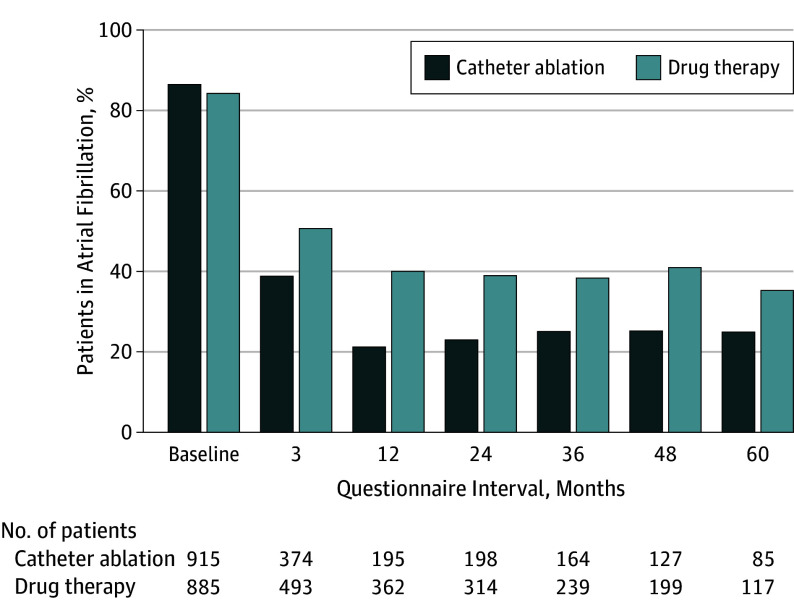
Results: Among 2204 randomized patients (median age, 68 years; 1385 patients [63%] were men, 946 [43%] had paroxysmal AF, and 1256 [57%] had persistent AF), the median follow-up was 48.5 months, and 1968 (89%) completed the trial. The mean AFEQT summary score was more favorable in the catheter ablation group than the drug therapy group at 12 months (86.4 points vs 80.9 points) (adjusted difference, 5.3 points [95% CI, 3.7-6.9]; P < .001). The mean MAFSI frequency score was more favorable for the catheter ablation group than the drug therapy group at 12 months (6.4 points vs 8.1 points) (adjusted difference, -1.7 points [95% CI, -2.3 to -1.2]; P < .001) and the mean MAFSI severity score was more favorable for the catheter ablation group than the drug therapy group at 12 months (5.0 points vs 6.5 points) (adjusted difference, -1.5 points [95% CI, -2.0 to -1.1]; P < .001).
Conclusions and relevance: Among patients with symptomatic atrial fibrillation, catheter ablation, compared with medical therapy, led to clinically important and significant improvements in quality of life at 12 months. These findings can help guide decisions regarding management of atrial fibrillation.
Trial registration: ClinicalTrials.gov Identifier: NCT00911508.
Conflict of interest statement
Figures
Comment in
-
Catheter Ablation for Atrial Fibrillation: Lessons Learned From CABANA.JAMA. 2019 Apr 2;321(13):1255-1257. doi: 10.1001/jama.2018.17478. JAMA. 2019. PMID: 30874732 No abstract available.
-
Catheter ablation improved quality of life more than drug therapy at 1 y in symptomatic atrial fibrillation.Ann Intern Med. 2019 Jul 16;171(2):JC9. doi: 10.7326/ACPJ201907160-009. Ann Intern Med. 2019. PMID: 31307070 No abstract available.
-
Atrial fibrillation and kidney disease: stuck outside the CABANA.Kidney Int. 2019 Nov;96(5):1054-1055. doi: 10.1016/j.kint.2019.05.023. Epub 2019 Jun 5. Kidney Int. 2019. PMID: 31443996 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
