

Risk Stratification in Differentiated Thyroid Cancer: From Detection to Final Follow-Up
- PMID: 30874735
- PMCID: PMC6684308
- DOI: 10.1210/jc.2019-00177
Risk Stratification in Differentiated Thyroid Cancer: From Detection to Final Follow-Up
Abstract
Context: Modern management of differentiated thyroid cancer requires individualized care plans that tailor the intensity of therapy and follow-up to the estimated risks of recurrence and disease-specific mortality.
Design: This summary is based on the authors' knowledge and extensive clinical experience, supplemented by review of published review articles, thyroid cancer management guidelines, published staging systems, and original articles identified through a PubMed search, which included terms such as risk stratification, staging, clinical outcomes, and differentiated thyroid cancer.
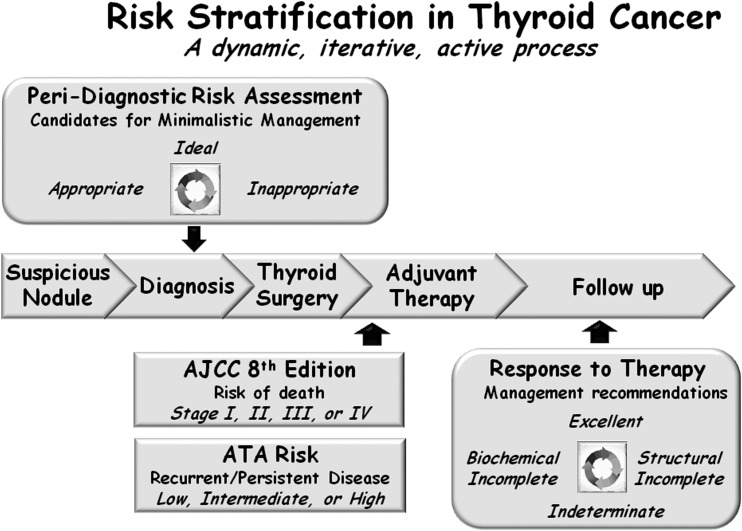
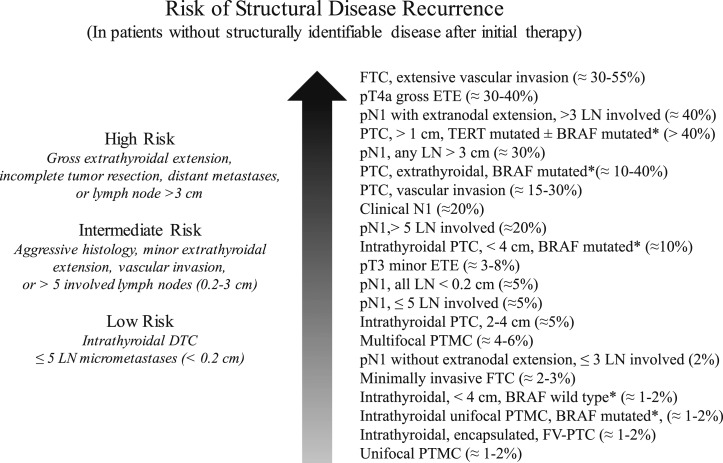
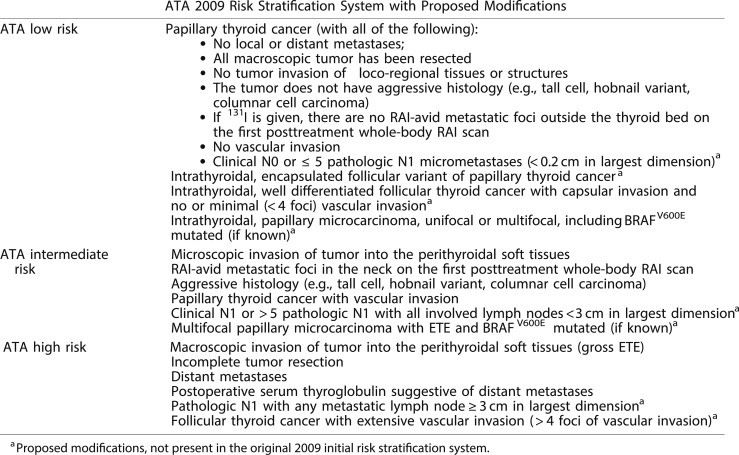
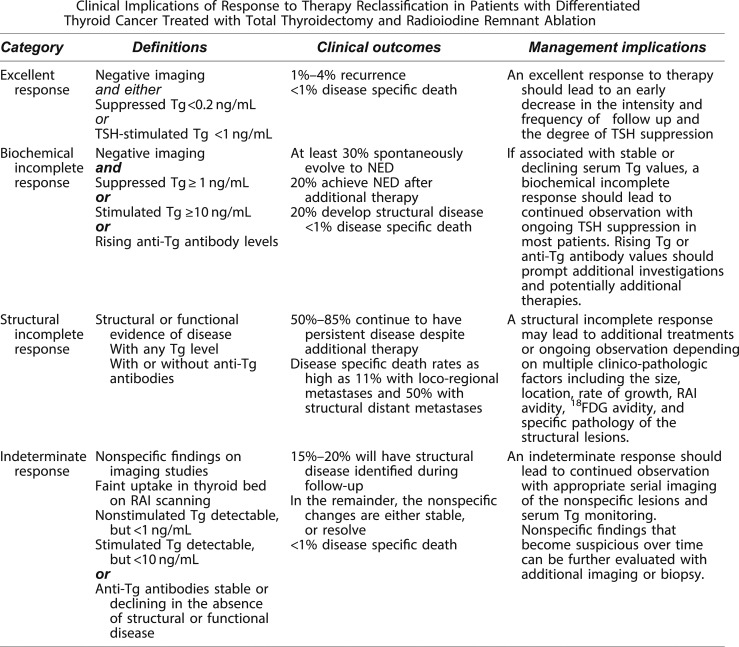
Main outcome measures: In the past, risk stratification in differentiated thyroid cancer usually referred to a static estimate of disease-specific mortality that was based on a small set of clinicopathological features available within a few weeks of completing initial therapy (thyroidectomy, with or without radioactive iodine). Today, risk stratification is a dynamic, active process used to predict the appropriateness for minimalistic initial therapy, disease-specific mortality, risk of recurrence, and the most likely response to initial therapy. Rather than being a static prediction available only after initial therapy, modern risk stratification is a dynamic, iterative process that begins as soon as a suspicious nodule is detected and continues through final follow-up.
Conclusions: Dynamic risk assessment should be used to guide all aspects of thyroid cancer management, beginning before a definitive diagnosis is made and continuing through the final follow-up visit.
Copyright © 2019 Endocrine Society.
Figures
References
-
- Brierley JD, Panzarella T, Tsang RW, Gospodarowicz MK, O’Sullivan B. A comparison of different staging systems predictability of patient outcome. Thyroid carcinoma as an example. Cancer. 1997;79(12):2414–2423. - PubMed
-
- Dean DS, Hay ID. Prognostic indicators in differentiated thyroid carcinoma. Cancer Contr. 2000;7(3):229–239. - PubMed
-
- Gillanders SL, O'Neill JP. Prognostic markers in well differentiated papillary and follicular thyroid cancer (WDTC). Eur J Surg Oncol. 2018;44(3):286–296. - PubMed
-
- Gilliland FD, Hunt WC, Morris DM, Key CR. Prognostic factors for thyroid carcinoma. A population-based study of 15,698 cases from the Surveillance, Epidemiology and End Results (SEER) program 1973–1991. Cancer. 1997;79(3):564–573. - PubMed
-
- Glikson E, Alon E, Bedrin L, Talmi YP. Prognostic factors in differentiated thyroid cancer revisited. Isr Med Assoc J. 2017;19(2):114–118. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
