

Levels of Evidence Supporting American College of Cardiology/American Heart Association and European Society of Cardiology Guidelines, 2008-2018
- PMID: 30874755
- PMCID: PMC6439920
- DOI: 10.1001/jama.2019.1122
Levels of Evidence Supporting American College of Cardiology/American Heart Association and European Society of Cardiology Guidelines, 2008-2018
Abstract
Importance: Clinical decisions are ideally based on evidence generated from multiple randomized controlled trials (RCTs) evaluating clinical outcomes, but historically, few clinical guideline recommendations have been based entirely on this type of evidence.
Objective: To determine the class and level of evidence (LOE) supporting current major cardiovascular society guideline recommendations, and changes in LOE over time.
Data sources: Current American College of Cardiology/American Heart Association (ACC/AHA) and European Society of Cardiology (ESC) clinical guideline documents (2008-2018), as identified on cardiovascular society websites, and immediate predecessors to these guideline documents (1999-2014), as referenced in current guideline documents.
Study selection: Comprehensive guideline documents including recommendations organized by class and LOE.
Data extraction and synthesis: The number of recommendations and the distribution of LOE (A [supported by data from multiple RCTs or a single, large RCT], B [supported by data from observational studies or a single RCT], and C [supported by expert opinion only]) were determined for each guideline document.
Main outcomes and measures: The proportion of guideline recommendations supported by evidence from multiple RCTs (LOE A).
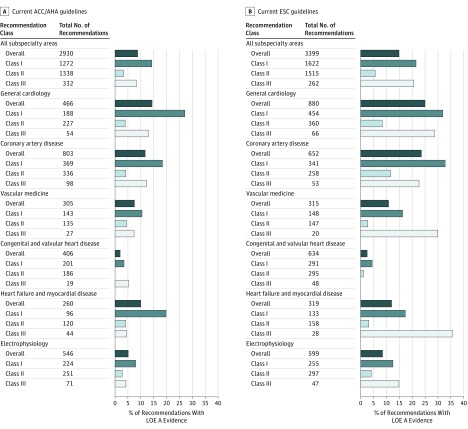
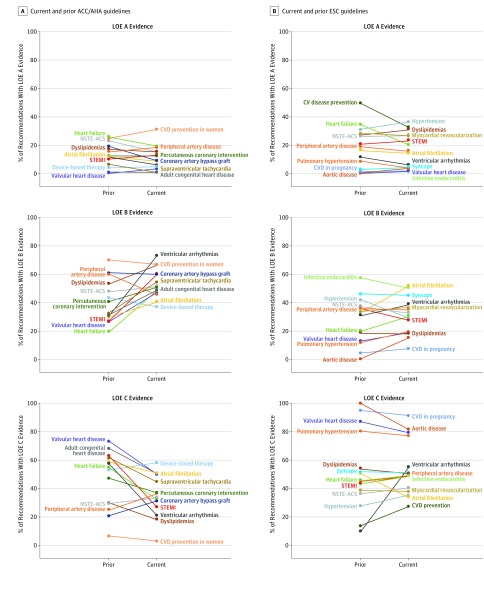
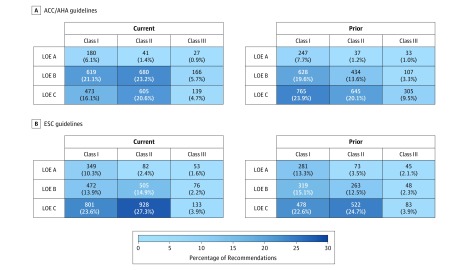
Results: Across 26 current ACC/AHA guidelines (2930 recommendations; median, 121 recommendations per guideline [25th-75th percentiles, 76-155]), 248 recommendations (8.5%) were classified as LOE A, 1465 (50.0%) as LOE B, and 1217 (41.5%) as LOE C. The median proportion of LOE A recommendations was 7.9% (25th-75th percentiles, 0.9%-15.2%). Across 25 current ESC guideline documents (3399 recommendations; median, 130 recommendations per guideline [25th-75th percentiles, 111-154]), 484 recommendations (14.2%) were classified as LOE A, 1053 (31.0%) as LOE B, and 1862 (54.8%) as LOE C. When comparing current guidelines with prior versions, the proportion of recommendations that were LOE A did not increase in either ACC/AHA (median, 9.0% [current] vs 11.7% [prior]) or ESC guidelines (median, 15.1% [current] vs 17.6% [prior]).
Conclusions and relevance: Among recommendations in major cardiovascular society guidelines, only a small percentage were supported by evidence from multiple RCTs or a single, large RCT. This pattern does not appear to have meaningfully improved from 2008 to 2018.
Conflict of interest statement
Figures

Comment in
-
The Evidence Supporting Cardiovascular Guidelines: Is There Evidence of Progress in the Last Decade?JAMA. 2019 Mar 19;321(11):1053-1054. doi: 10.1001/jama.2019.2018. JAMA. 2019. PMID: 30874738 No abstract available.
References
-
- Mehta RH, Chen AY, Alexander KP, Ohman EM, Roe MT, Peterson ED. Doing the right things and doing them the right way: association between hospital guideline adherence, dosing safety, and outcomes among patients with acute coronary syndrome. Circulation. 2015;131(11):980-987. doi: 10.1161/CIRCULATIONAHA.114.013451 - DOI - PubMed
-
- Komajda M, Cowie MR, Tavazzi L, Ponikowski P, Anker SD, Filippatos GS; QUALIFY Investigators . Physicians’ guideline adherence is associated with better prognosis in outpatients with heart failure with reduced ejection fraction: the QUALIFY international registry. Eur J Heart Fail. 2017;19(11):1414-1423. doi: 10.1002/ejhf.887 - DOI - PubMed
-
- Lip GY, Laroche C, Popescu MI, et al. Improved outcomes with European Society of Cardiology guideline-adherent antithrombotic treatment in high-risk patients with atrial fibrillation: a report from the EORP-AF General Pilot Registry. Europace. 2015;17(12):1777-1786. doi: 10.1093/europace/euv269 - DOI - PubMed
