

Associations of Dietary Cholesterol or Egg Consumption With Incident Cardiovascular Disease and Mortality
- PMID: 30874756
- PMCID: PMC6439941
- DOI: 10.1001/jama.2019.1572
Associations of Dietary Cholesterol or Egg Consumption With Incident Cardiovascular Disease and Mortality
Abstract
Importance: Cholesterol is a common nutrient in the human diet and eggs are a major source of dietary cholesterol. Whether dietary cholesterol or egg consumption is associated with cardiovascular disease (CVD) and mortality remains controversial.
Objective: To determine the associations of dietary cholesterol or egg consumption with incident CVD and all-cause mortality.
Design, setting, and participants: Individual participant data were pooled from 6 prospective US cohorts using data collected between March 25, 1985, and August 31, 2016. Self-reported diet data were harmonized using a standardized protocol.
Exposures: Dietary cholesterol (mg/day) or egg consumption (number/day).
Main outcomes and measures: Hazard ratio (HR) and absolute risk difference (ARD) over the entire follow-up for incident CVD (composite of fatal and nonfatal coronary heart disease, stroke, heart failure, and other CVD deaths) and all-cause mortality, adjusting for demographic, socioeconomic, and behavioral factors.
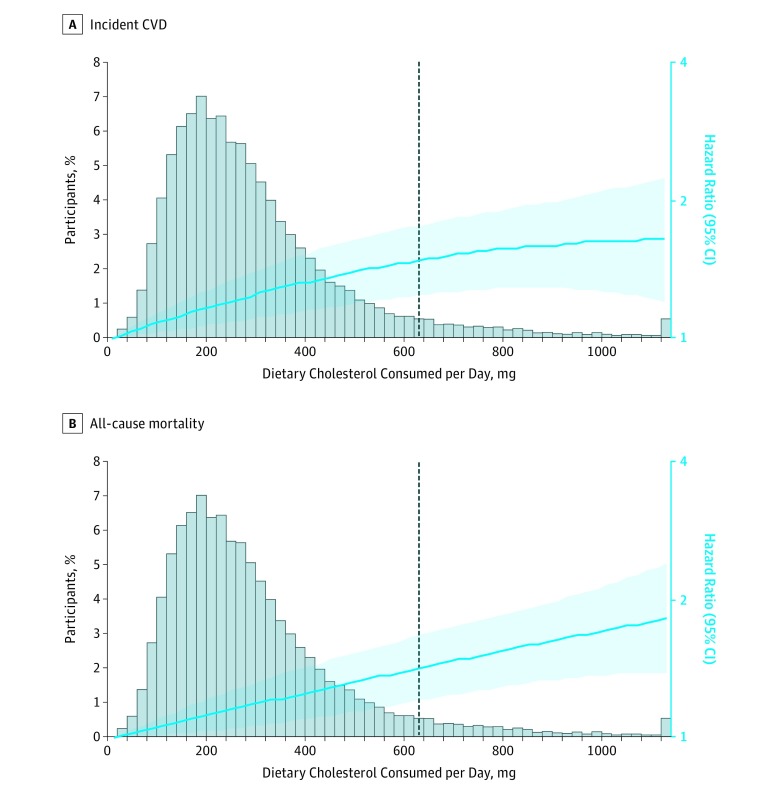
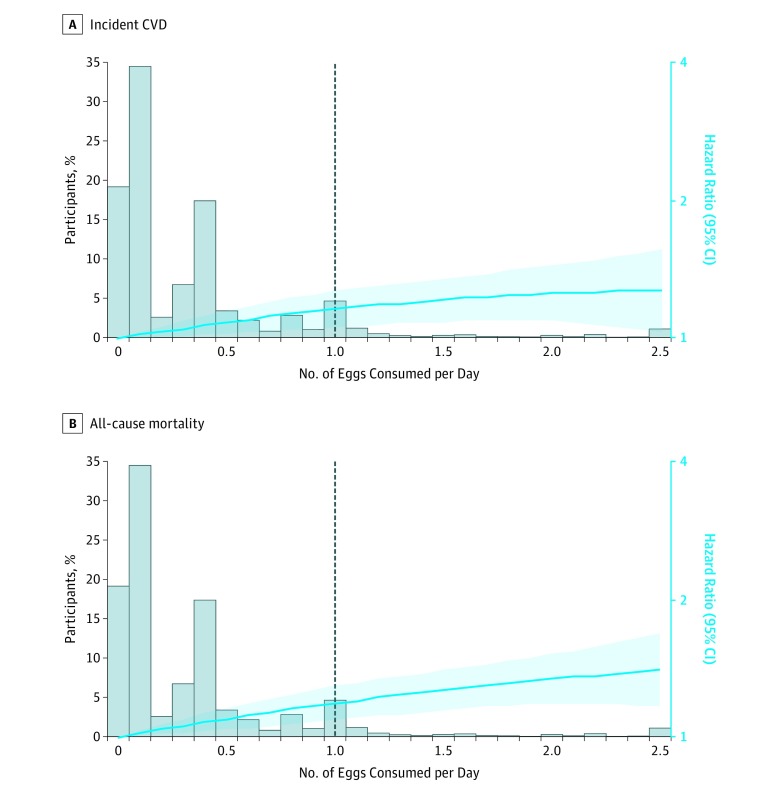
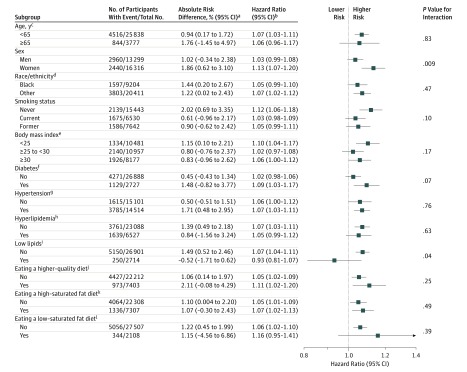
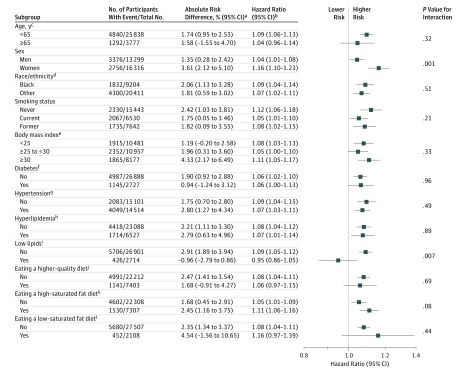
Results: This analysis included 29 615 participants (mean [SD] age, 51.6 [13.5] years at baseline) of whom 13 299 (44.9%) were men and 9204 (31.1%) were black. During a median follow-up of 17.5 years (interquartile range, 13.0-21.7; maximum, 31.3), there were 5400 incident CVD events and 6132 all-cause deaths. The associations of dietary cholesterol or egg consumption with incident CVD and all-cause mortality were monotonic (all P values for nonlinear terms, .19-.83). Each additional 300 mg of dietary cholesterol consumed per day was significantly associated with higher risk of incident CVD (adjusted HR, 1.17 [95% CI, 1.09-1.26]; adjusted ARD, 3.24% [95% CI, 1.39%-5.08%]) and all-cause mortality (adjusted HR, 1.18 [95% CI, 1.10-1.26]; adjusted ARD, 4.43% [95% CI, 2.51%-6.36%]). Each additional half an egg consumed per day was significantly associated with higher risk of incident CVD (adjusted HR, 1.06 [95% CI, 1.03-1.10]; adjusted ARD, 1.11% [95% CI, 0.32%-1.89%]) and all-cause mortality (adjusted HR, 1.08 [95% CI, 1.04-1.11]; adjusted ARD, 1.93% [95% CI, 1.10%-2.76%]). The associations between egg consumption and incident CVD (adjusted HR, 0.99 [95% CI, 0.93-1.05]; adjusted ARD, -0.47% [95% CI, -1.83% to 0.88%]) and all-cause mortality (adjusted HR, 1.03 [95% CI, 0.97-1.09]; adjusted ARD, 0.71% [95% CI, -0.85% to 2.28%]) were no longer significant after adjusting for dietary cholesterol consumption.
Conclusions and relevance: Among US adults, higher consumption of dietary cholesterol or eggs was significantly associated with higher risk of incident CVD and all-cause mortality in a dose-response manner. These results should be considered in the development of dietary guidelines and updates.
Conflict of interest statement
Figures




Comment in
-
Reconsidering the Importance of the Association of Egg Consumption and Dietary Cholesterol With Cardiovascular Disease Risk.JAMA. 2019 Mar 19;321(11):1055-1056. doi: 10.1001/jama.2019.1850. JAMA. 2019. PMID: 30874737 No abstract available.
-
Egg consumption: to eat or not to eat?J Thorac Dis. 2019 Jun;11(6):2185-2187. doi: 10.21037/jtd.2019.06.21. J Thorac Dis. 2019. PMID: 31372247 Free PMC article. No abstract available.
-
Editor's note: Alcohol consumption and health: An ongoing debate.Nutr Metab Cardiovasc Dis. 2019 Oct;29(10):1001-1002. doi: 10.1016/j.numecd.2019.07.005. Epub 2019 Jul 9. Nutr Metab Cardiovasc Dis. 2019. PMID: 31378625 No abstract available.
-
Dietary Cholesterol or Egg Consumption and Cardiovascular Outcomes.JAMA. 2019 Aug 6;322(5):466-467. doi: 10.1001/jama.2019.7220. JAMA. 2019. PMID: 31386127 No abstract available.
References
-
- Berger S, Raman G, Vishwanathan R, Jacques PF, Johnson EJ. Dietary cholesterol and cardiovascular disease. Am J Clin Nutr. 2015;102(2):276-294. - PubMed
-
- US Department of Health and Human Services and US Department of Agriculture 2015-2020 Dietary Guidelines for Americans. 8th Edition. December 2015. https://health.gov/dietaryguidelines/2015/guidelines/. Accessed January 31, 2019.
-
- Dietary Guidelines Advisory Committee Scientific Report of the 2015 Dietary Guidelines Advisory Committee: Advisory Report to the Secretary of Health and Human Services and the Secretary of Agriculture. Washington, DC: US Dept of Agriculture, Agricultural Research Service; 2015.
-
- US Department of Agriculture Agricultural Research Service, Nutrient Data Laboratory. USDA National Nutrient Database for Standard Reference, Release 28. Version Current: September 2015. https://ndb.nal.usda.gov/ndb/. Accessed January 31, 2019.
