

Association of Light Physical Activity Measured by Accelerometry and Incidence of Coronary Heart Disease and Cardiovascular Disease in Older Women
- PMID: 30874775
- PMCID: PMC6484645
- DOI: 10.1001/jamanetworkopen.2019.0419
Association of Light Physical Activity Measured by Accelerometry and Incidence of Coronary Heart Disease and Cardiovascular Disease in Older Women
Erratum in
-
Typographical Error in Conclusions.JAMA Netw Open. 2019 May 3;2(5):e194476. doi: 10.1001/jamanetworkopen.2019.4476. JAMA Netw Open. 2019. PMID: 31074801 Free PMC article. No abstract available.
Abstract
Importance: To our knowledge, no studies have examined light physical activity (PA) measured by accelerometry and heart disease in older women.
Objective: To investigate whether higher levels of light PA were associated with reduced risks of coronary heart disease (CHD) or cardiovascular disease (CVD) in older women.
Design, setting, and participants: Prospective cohort study of older women from baseline (March 2012 to April 2014) through February 28, 2017, for up to 4.91 years. The setting was community-dwelling participants from the Women's Health Initiative. Participants were ambulatory women with no history of myocardial infarction or stroke.
Exposures: Data from accelerometers worn for a requested 7 days were used to measure light PA.
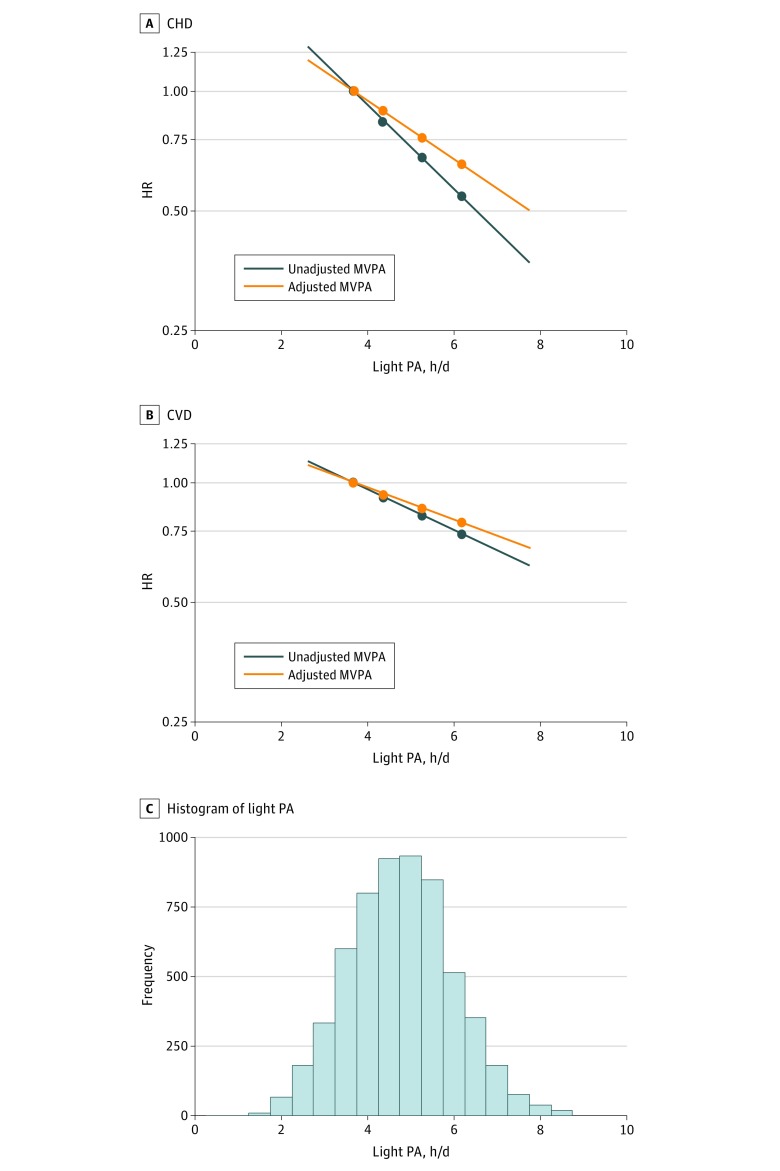
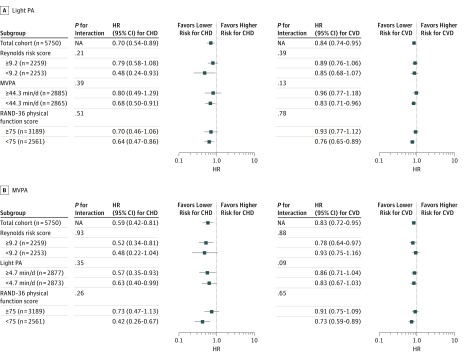
Main outcomes and measures: Cox proportional hazards regression models estimated hazard ratios (HRs) and 95% CIs for physician-adjudicated CHD and CVD events across light PA quartiles adjusting for possible confounders. Light PA was also analyzed as a continuous variable with and without adjustment for moderate to vigorous PA (MVPA).
Results: Among 5861 women (mean [SD] age, 78.5 [6.7] years), 143 CHD events and 570 CVD events were observed. The HRs for CHD in the highest vs lowest quartiles of light PA were 0.42 (95% CI, 0.25-0.70; P for trend <.001) adjusted for age and race/ethnicity and 0.58 (95% CI, 0.34-0.99; P for trend = .004) after additional adjustment for education, current smoking, alcohol consumption, physical functioning, comorbidity, and self-rated health. Corresponding HRs for CVD in the highest vs lowest quartiles of light PA were 0.63 (95% CI, 0.49-0.81; P for trend <.001) and 0.78 (95% CI, 0.60-1.00; P for trend = .004). The HRs for a 1-hour/day increment in light PA after additional adjustment for MVPA were 0.86 (95% CI, 0.73-1.00; P for trend = .05) for CHD and 0.92 (95% CI, 0.85-0.99; P for trend = .03) for CVD.
Conclusions and relevance: The present findings support the conclusion that all movement counts for the prevention of CHD and CVD in older women. Large, pragmatic randomized trials are needed to test whether increasing light PA among older women reduces cardiovascular risk.
Conflict of interest statement
Figures
Comment in
-
Light Physical Activity and Incident Coronary Heart Disease and Cardiovascular Disease Among Older Women-A Call for Action.JAMA Netw Open. 2019 Mar 1;2(3):e190405. doi: 10.1001/jamanetworkopen.2019.0405. JAMA Netw Open. 2019. PMID: 30874773 No abstract available.
References
-
- Mehta LS, Beckie TM, DeVon HA, et al. ; American Heart Association Cardiovascular Disease in Women and Special Populations Committee of the Council on Clinical Cardiology, Council on Epidemiology and Prevention, Council on Cardiovascular and Stroke Nursing, and Council on Quality of Care and Outcomes Research . Acute myocardial infarction in women: a scientific statement from the American Heart Association. Circulation. 2016;133(9):-. doi: 10.1161/CIR.0000000000000351 - DOI - PubMed
-
- National Center for Health Statistics Health, United States, 2016: With Chartbook on Long-term Trends in Health. Hyattsville, MD: National Center for Health Statistics; May 2017. - PubMed
-
- Wilmot KA, O’Flaherty M, Capewell S, Ford ES, Vaccarino V. Coronary heart disease mortality declines in the United States from 1979 through 2011: evidence for stagnation in young adults, especially women. Circulation. 2015;132(11):997-1002. doi: 10.1161/CIRCULATIONAHA.115.015293 - DOI - PMC - PubMed
-
- Benjamin EJ, Blaha MJ, Chiuve SE, et al. ; American Heart Association Statistics Committee and Stroke Statistics Subcommittee . Heart disease and stroke statistics–2017 update: a report from the American Heart Association [published corrections appears in Circulation. 2017;135(10):e646 and 2017;136(10):e196]. Circulation. 2017;135(10):e146-e603. doi: 10.1161/CIR.0000000000000485 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
