

Twenty-Year Trends in Outcomes for Older Adults With Acute Myocardial Infarction in the United States
- PMID: 30874787
- PMCID: PMC6484647
- DOI: 10.1001/jamanetworkopen.2019.1938
Twenty-Year Trends in Outcomes for Older Adults With Acute Myocardial Infarction in the United States
Abstract
Importance: Medicare and other organizations have focused on improving quality of care for patients with acute myocardial infarction (AMI) over the last 2 decades. However, there is no comprehensive perspective on the evolution of outcomes for AMI during that period, and it is unknown whether temporal changes varied by patient subgroup, hospital, or county.
Objective: To provide a comprehensive evaluation of national trends in inpatient outcomes and costs of AMI during this period.
Design, setting, and participants: This cohort study included analysis of data from a sample of 4 367 485 Medicare fee-for-service beneficiaries aged 65 years or older from January 1, 1995, through December 31, 2014, across 5680 hospitals in the United States. Analyses were conducted from January 15 to June 5, 2018.
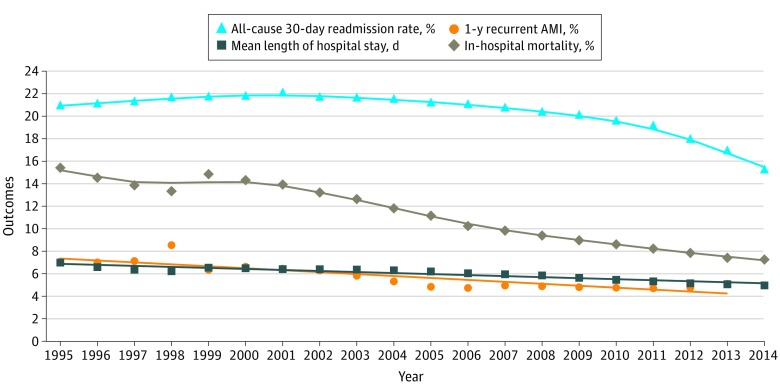
Main outcomes and measures: Thirty-day all-cause mortality at the patient, hospital, and county levels. Additional outcomes included 30-day all-cause readmissions; 1-year recurrent AMI; in-hospital mortality; length of hospital stay; 2014 Consumer Price Index-adjusted median Medicare inpatient payment per AMI discharge; and rates of catheterization, percutaneous coronary intervention, and coronary artery bypass graft surgery.
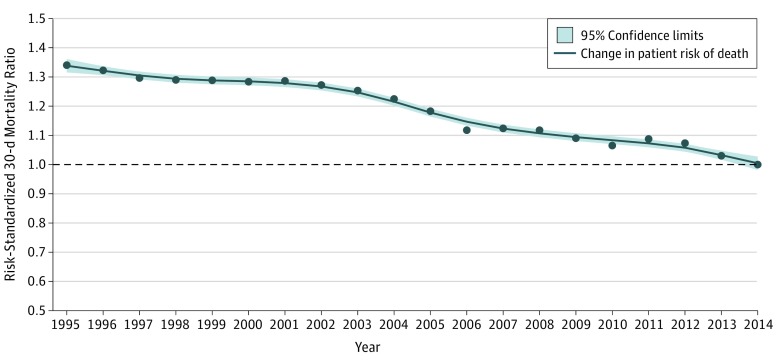
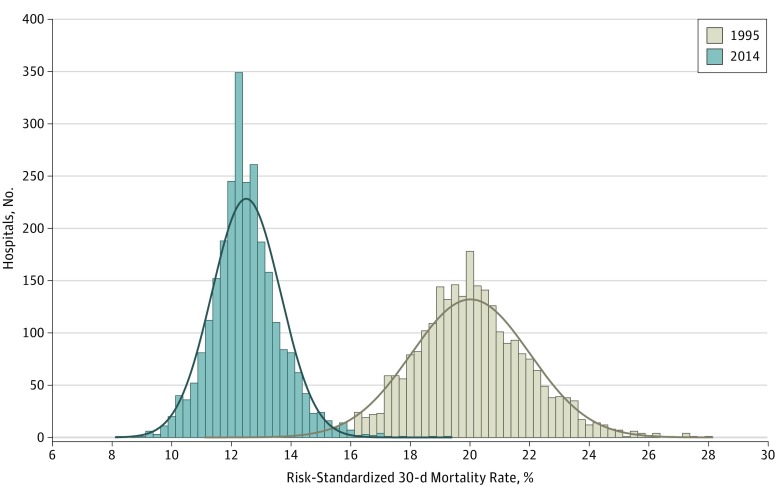
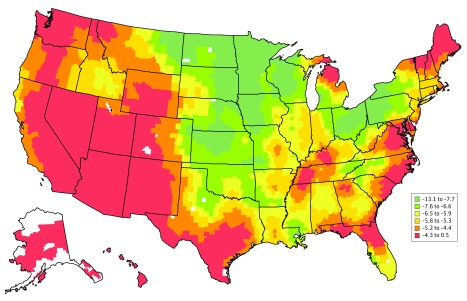
Results: The cohort included 4 367 485 Medicare fee-for-service patients aged 65 years or older hospitalized for AMI during the study period. Between 1995 and 2014, the mean (SD) age of patients increased from 76.9 (7.2) to 78.2 (8.7) years, the percentage of female patients declined from 49.5% to 46.1%, the percentage of white patients declined from 91.0% to 86.2%, and the percentage of black patients increased from 5.9% to 8.0%. There were declines in AMI hospitalizations (914 to 566 per 100 000 beneficiary-years); 30-day mortality (20.0% to 12.4%; difference, 7.6 percentage points; 95% CI, 7.3-7.8 percentage points); 30-day all-cause readmissions (21.0% to 15.3%; difference, 5.7 percentage points; 95% CI, 5.4-6.0 percentage points); and 1-year recurrent AMI (7.1% to 5.1%; difference, 2.0 percentage points; 95% CI, 1.8-2.2 percentage points). There were increases in the 2014 Consumer Price Index-adjusted median (interquartile range) Medicare inpatient payment per AMI discharge ($9282 [$6969-$12 173] to $11 031 [$8099-$16 861]); 30-day inpatient catheterization (44.2% to 59.9%; difference, 15.7 percentage points; 95% CI, 15.4-16.0 percentage points); and inpatient percutaneous coronary intervention (18.8% to 43.3%; difference, 24.5 percentage points; 95% CI, 24.2-24.7 percentage points). Coronary artery bypass graft surgery rates decreased from 14.4% to 10.2% (difference, 4.2 percentage points; 95% CI, 3.9-4.3 percentage points). There was heterogeneity by hospital and county in the mortality changes over time.
Conclusions and relevance: This study shows marked improvements in short-term mortality and readmissions, with an increase in in-hospital procedures and payments, for the increasingly smaller number of Medicare beneficiaries with AMI.
Conflict of interest statement
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
