

Machine perfusion preservation versus static cold storage for deceased donor kidney transplantation
- PMID: 30875082
- PMCID: PMC6419919
- DOI: 10.1002/14651858.CD011671.pub2
Machine perfusion preservation versus static cold storage for deceased donor kidney transplantation
Update in
-
Normothermic and hypothermic machine perfusion preservation versus static cold storage for deceased donor kidney transplantation.Cochrane Database Syst Rev. 2024 Jul 9;7(7):CD011671. doi: 10.1002/14651858.CD011671.pub3. Cochrane Database Syst Rev. 2024. PMID: 38979743 Free PMC article.
Abstract
Background: Kidney transplantation is the optimal treatment for end-stage kidney disease. Retrieval, transport and transplant of kidney grafts causes ischaemia reperfusion injury. The current accepted standard is static cold storage (SCS) whereby the kidney is stored on ice after removal from the donor and then removed from the ice box at the time of implantation. However, technology is now available to perfuse or "pump" the kidney during the transport phase or at the recipient centre. This can be done at a variety of temperatures and using different perfusates. The effectiveness of treatment is manifest clinically as delayed graft function (DGF), whereby the kidney fails to produce urine immediately after transplant.
Objectives: To compare hypothermic machine perfusion (HMP) and (sub)normothermic machine perfusion (NMP) with standard SCS.
Search methods: We searched the Cochrane Kidney and Transplant Register of Studies to 18 October 2018 through contact with the Information Specialist using search terms relevant to this review. Studies in the Register are identified through searches of CENTRAL, MEDLINE, and EMBASE, conference proceedings, the International Clinical Trials Register (ICTRP) Search Portal and ClinicalTrials.gov.
Selection criteria: All randomised controlled trials (RCTs) and quasi-RCTs comparing HMP/NMP versus SCS for deceased donor kidney transplantation were eligible for inclusion. All donor types were included (donor after circulatory (DCD) and brainstem death (DBD), standard and extended/expanded criteria donors). Both paired and unpaired studies were eligible for inclusion.
Data collection and analysis: The results of the literature search were screened and a standard data extraction form was used to collect data. Both of these steps were performed by two independent authors. Dichotomous outcome results were expressed as risk ratio (RR) with 95% confidence intervals (CI). Continuous scales of measurement were expressed as a mean difference (MD). Random effects models were used for data analysis. The primary outcome was incidence of DGF. Secondary outcomes included: one-year graft survival, incidence of primary non-function (PNF), DGF duration, long term graft survival, economic implications, graft function, patient survival and incidence of acute rejection.
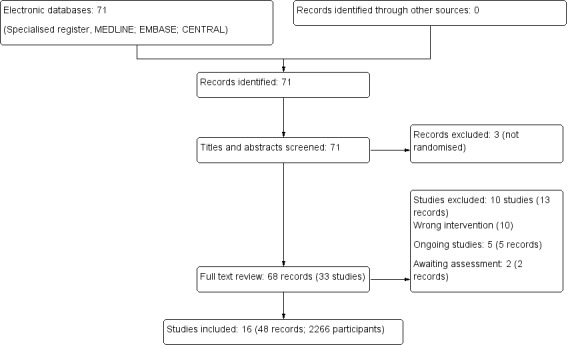
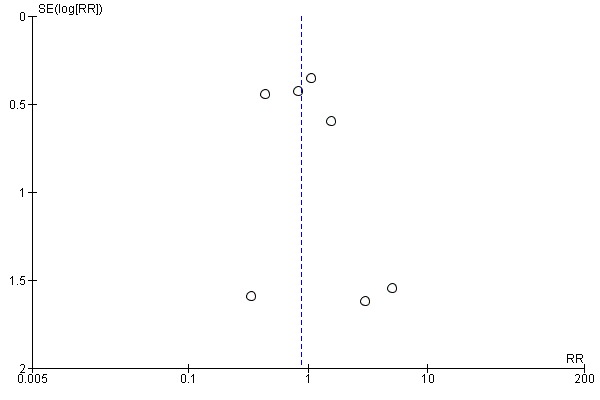
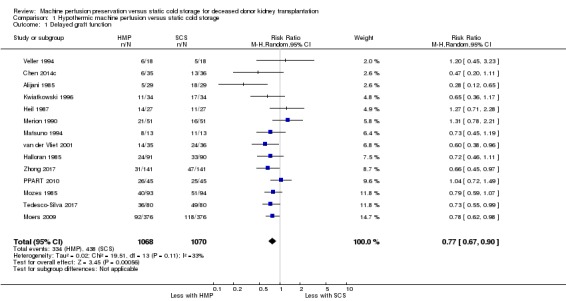
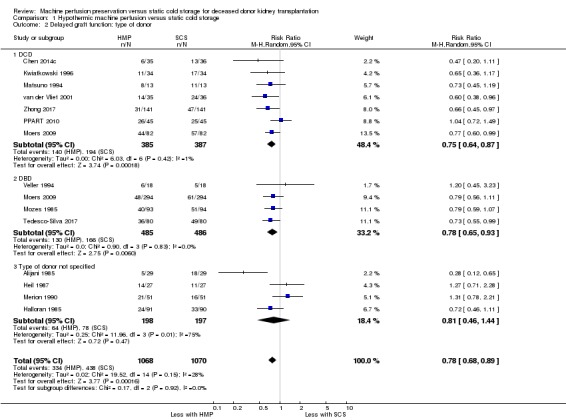
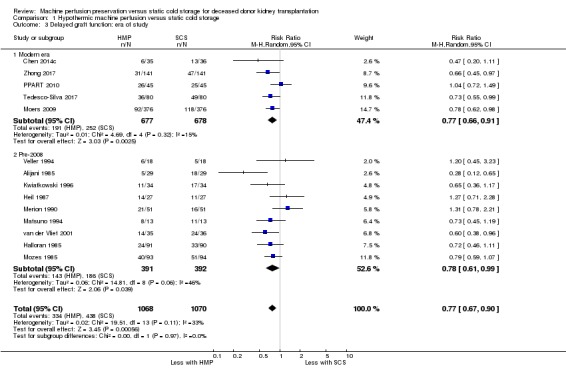
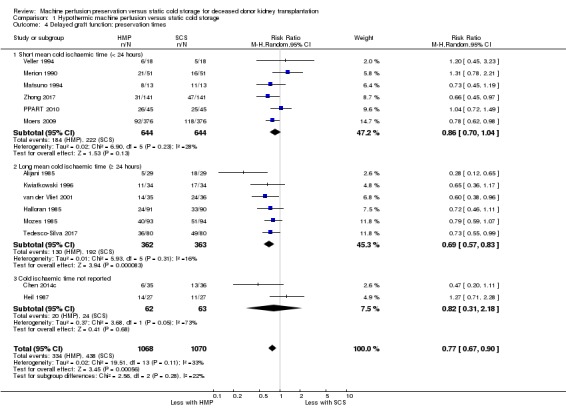
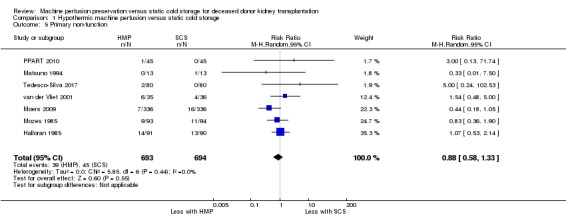
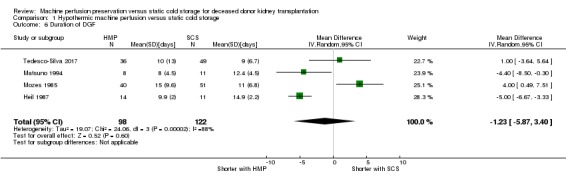
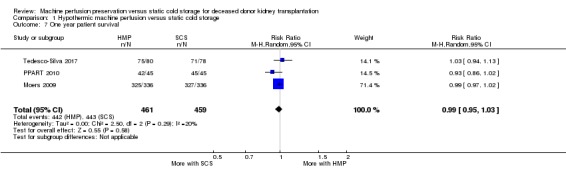
Main results: No studies reported on NMP, however one ongoing study was identified.Sixteen studies (2266 participants) comparing HMP with SCS were included; 15 studies could be meta-analysed. Fourteen studies reported on requirement for dialysis in the first week post-transplant (DGF incidence); there is high-certainty evidence that HMP reduces the risk of DGF when compared to SCS (RR 0.77; 95% CI 0.67 to 0.90; P = 0.0006). HMP reduces the risk of DGF in kidneys from DCD donors (7 studies, 772 participants: RR 0.75; 95% CI 0.64 to 0.87; P = 0.0002; high certainty evidence), as well as kidneys from DBD donors (4 studies, 971 participants: RR 0.78, 95% CI 0.65 to 0.93; P = 0.006; high certainty evidence). The number of perfusions required to prevent one episode of DGF (number needed to treat, NNT) was 7.26 and 13.60 in DCD and DBD kidneys respectively. Studies performed in the last decade all used the LifePort machine and confirmed that HMP reduces the incidence of DGF in the modern era (5 studies, 1355 participants: RR 0.77, 95% CI 0.66 to 0.91; P = 0.002; high certainty evidence). Reports of economic analysis suggest that HMP can lead to cost savings in both the North American and European settings.Two studies reported HMP also improves graft survival however we were not able to meta-analyse these results. A reduction in incidence of PNF could not be demonstrated. The effect of HMP on our other outcomes (incidence of acute rejection, patient survival, hospital stay, long-term graft function, duration of DGF) remains uncertain.
Authors' conclusions: HMP is superior to SCS in deceased donor kidney transplantation. This is true for both DBD and DCD kidneys, and remains true in the modern era (studies performed in the last decade). As kidneys from DCD donors have a higher overall DGF rate, fewer perfusions are needed to prevent one episode of DGF (7.26 versus 13.60 in DBD kidneys).Further studies looking solely at the impact of HMP on DGF incidence are not required. Follow-up reports detailing long-term graft survival from participants of the studies already included in this review would be an efficient way to generate further long-term graft survival data.Economic analysis, based on the results of this review, would help cement HMP as the standard preservation method in deceased donor kidney transplantation.RCTs investigating (sub)NMP are required.
Conflict of interest statement
Samuel J Tingle: none known
Rodrigo S Figueiredo: none known
John AG Moir: none known
Michael Goodfellow: none known
David Talbot: essentially none, but I have received help in attending transplant meetings in the past. This has usually come from one of four companies (Astellas, Wyeth, Novartis and Roche)
Colin H Wilson: none known
Figures
References
References to studies included in this review
-
- Alijani MR, Cutler JA, DelValle CJ, Morres DN, Fawzy A, Pechan BW, et al. Single‐donor cold storage versus machine perfusion in cadaver kidney preservation. Transplantation 1985;40(6):659‐61. [MEDLINE: ] - PubMed
-
- Amaduzzi A, Catena F, Montori G, Ravaioli M, Pinna A. Hypotermic machine perfusion (HMP) versus static cold storage (CS) in kidney allograft preservation. Prospective case‐control trial [abstract no: RO‐077]. Transplant International 2011;24(Suppl 2):151. [EMBASE: 70527605]
-
- Chen G, Ko D, Wang C, Yuan X, Qiu J, Han M, et al. Impact of machine perfusion on outcomes of kidney transplantation from donation after cardiac death: a prospective randomized controlled trial [abstract no: D2675]. Transplantation 2014;98(Suppl 1):267. [EMBASE: 71544357]
-
- Halloran P, Aprile M. A randomized prospective trial of cold storage versus pulsatile perfusion for cadaver kidney preservation. Transplantation 1987;43(6):827‐32. [MEDLINE: ] - PubMed
- Halloran P, Aprile M, Robinette M. A randomized prospective trial of cold storage versus pulsatile perfusion for cadaver kidney preservation. Transplantation Proceedings 1985;17(1 Part 2):1471‐3. [EMBASE: 1985080743] - PubMed
-
- Heil JE, Canafax DM, Sutherland DE, Simmons RL, Dunning M, Najarian JS. A controlled comparison of kidney preservation by two methods: machine perfusion and cold storage. Transplantation Proceedings 1987;19(1 Pt 3):2046. [MEDLINE: ] - PubMed
References to studies excluded from this review
-
- Alijani MR, Helfrich GB, Fawzy A, Cutler JA, Bates SB, Andrews PM. Clinical evaluation of a new kidney cold storage solution [abstract]. Kidney International 1987;31(1):453. [CENTRAL: CN‐00550449]
-
- Baatard R, Pradier F, Dantal J, Karam G, Cantarovich D, Hourmant M, et al. Prospective randomized comparison of University of Wisconsin and UW‐modified, lacking hydroxyethyl‐starch, cold‐storage solutions in kidney transplantation. Transplantation 1993;55(1):31‐5. [MEDLINE: ] - PubMed
-
- Guarrera JV, Polyak M, O'Mar AB, Kapur S, Stubenbord WT, Kinkhabwala M. Pulsatile machine perfusion with Vasosol solution improves early graft function after cadaveric renal transplantation.[Retraction in Stubenbord WT, Kinkhabwala M, Kapur S. Transplantation. 2005 Jun 27;79(12):1774; PMID: 15973193]. Transplantation 2004;77(8):1264‐8. [MEDLINE: ] - PubMed
-
- Guarrera JV, Polyak MM, Arrington B, Boykin J, Brown T, Jean‐Jacques MA, et al. Pushing the envelope in renal preservation; improved results with novel perfusate modifications for pulsatile machine perfusion of cadaver kidneys.[Erratum appears in Transplant Proc. 2004 Jul‐Aug;36(6):1853 Note: O'Mar Arrington, B [corrected to Arrington, B]]. Transplantation Proceedings 2004;36(5):1257‐60. [MEDLINE: ] - PubMed
-
- Lodge JP, Kashi SH, Lam FT, Lord A, Giles GR. The reflush effect‐‐a prospective analysis of late perfusion. Transplantation 1993;55(3):567‐72. [MEDLINE: ] - PubMed
References to studies awaiting assessment
-
- Watson C. CArdiac Death kidney Machine Perfusion trial. www.isrctn.com/ISRCTN50082383 (first received 6 September 2011).
-
- NCT01170910. Pulsatile perfusion preservation in kidney transplantation from expanded criteria donors (IMPULSION). www.clinicaltrials.gov/ct2/show/NCT01170910 (first received 27 July 2010).
References to ongoing studies
-
- Hosgood SA, Saeb‐Parsy K, Wilson C, Callaghan C, Collett D, Nicholson ML. Protocol of a randomised controlled, open‐label trial of ex vivo normothermic perfusion versus static cold storage in donation after circulatory death renal transplantation. BMJ Open 2017;7(1):e012237. [MEDLINE: ] - PMC - PubMed
-
- Watson C. A multi‐centre, randomised, controlled study of pre‐transplant machine perfusion of heart‐beating donor kidneys prior to renal transplantation (HBDPump 2005). www.isrctn.com/ISRCTN35082773 (first received 10 May 2005).
-
- Paul A. COPE‐POMP: ‘in house’ pre‐implantation oxygenated hypothermic machine perfusion reconditioning after cold storage versus cold storage alone in expanded criteria donor (ECD) kidneys from brain dead donors. www.isrctn.com/ISRCTN63852508 (first received 28 February 2014).
-
- Malinoski D. Deceased organ donor interventions to protect kidney graft function. www.clinicaltrials.gov/ct2/show/NCT02525510 (first received 17 August 2015).
-
- Ding C. Clinical impact of hypothermic machine perfusion in renal transplant recipients (CIHMP). www.clinicaltrials.gov/ct2/show/NCT02621281 (first received 3 December 2015).
Additional references
-
- Bagul A, Hosgood SA, Kaushik M, Kay MD, Waller HL, Nicholson ML. Experimental renal preservation by normothermic resuscitation perfusion with autologous blood. British Journal of Surgery 2008;95(1):111‐8. [MEDLINE: ] - PubMed
-
- Belzer FO, Ashby BS, Gulyassy PF, Powell M. Successful seventeen‐hour preservation and transplantation of human‐cadaver kidney. New England Journal of Medicine 1968;278(11):608‐10. [MEDLINE: ] - PubMed
-
- Collins GM, Bravo‐Shugarman M, Terasaki PI. Kidney preservation for transportation. Initial perfusion and 30 hours' ice storage. Lancet 1969;2(7632):1219‐22. [MEDLINE: ] - PubMed
-
- Fresenius Medical Care. ESRD patients in 2013: a global perspective. Fresenius, Bad Homburg, Germany. www.vision‐fmc.com/files/ESRD_Patients_in_2013.pdf (last accessed 20 April 2015).
-
- Furukawa TA, Barbui C, Cipriani A, Brambilla P, Watanabe N. Imputing missing standard deviations in meta‐analyses can provide accurate results. Journal of Clinical Epidemiology 2006;59(1):7‐10. [MEDLINE: ] - PubMed
References to other published versions of this review
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials