

Atrial fibrillation ablation in practice: assessing CABANA generalizability
- PMID: 30875424
- PMCID: PMC6475520
- DOI: 10.1093/eurheartj/ehz085
Atrial fibrillation ablation in practice: assessing CABANA generalizability
Abstract
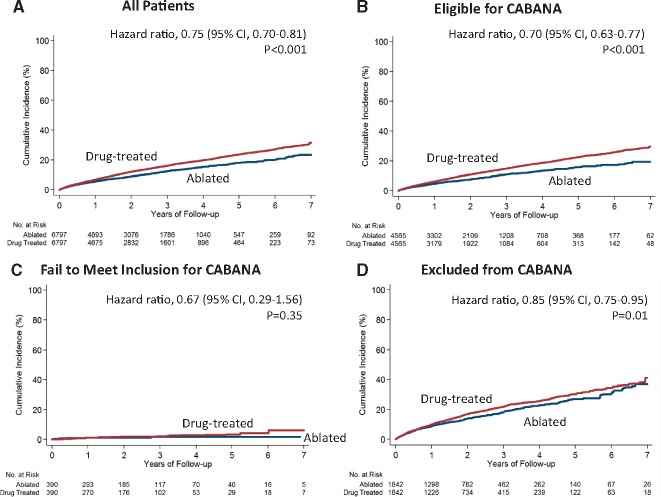
Aims: The Catheter Ablation vs. Antiarrhythmic Drug Therapy for Atrial Fibrillation (CABANA) trial aimed to assess the impact of ablation on morbidity and mortality. This observational study was conducted in parallel to CABANA to assess trial generalizability.
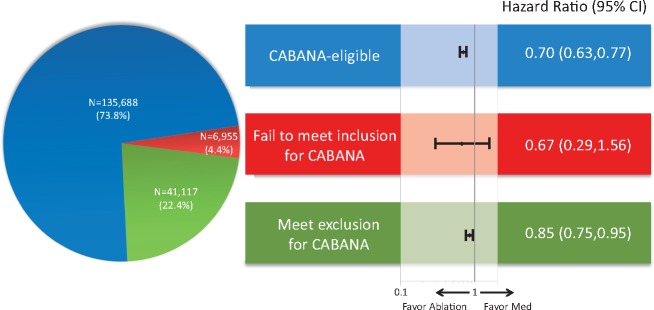
Methods and results: Using a large US administrative database, we identified 183 760 patients with atrial fibrillation (AF) treated with ablation or medical therapy (antiarrhythmic or rate control drugs) between 1 August 2009 and 30 April 2016 (CABANA enrolment period). Propensity score weighting was used to balance patients treated with ablation (N = 12 032) or medical therapy alone (N = 171 728) on 90 dimensions. Ablation was associated with a reduction in the composite endpoint of all-cause mortality, stroke, major bleeding, and cardiac arrest [hazard ratio (HR) 0.75, 95% confidence interval (CI) 0.70-0.81; P < 0.001]. The majority of patients (73.8%) were potentially trial eligible; among whom the risk reduction associated with ablation was greatest (HR 0.70, 95% CI 0.63-0.77; P < 0.001). Among the 3.8% of patients who failed to meet the inclusion criterion, i.e. patients under 65 years without stroke risk factors, the event rates were low and there was no significant relationship with ablation (HR 0.67, 95% CI 0.29-1.56; P = 0.35). Among the 22.4% patients who met at least one of the trial exclusion criteria, there was a lesser but statistically significant reduction associated with ablation (HR 0.85, 95% CI 0.75-0.95; P = 0.01).
Conclusion: In routine clinical care, ablation was associated with a reduction in the primary CABANA composite endpoint of all-cause mortality, stroke, major bleeding, and cardiac arrest, particularly in patients who were eligible for the trial.
Keywords: Ablation; Atrial fibrillation; Mortality; Stroke.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2019. For permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
Left atrial ablation for management of atrial fibrillation: CABANA vs. real-world data. Apples and oranges?Eur Heart J. 2019 Apr 21;40(16):1265-1267. doi: 10.1093/eurheartj/ehz168. Eur Heart J. 2019. PMID: 30875420 No abstract available.
References
-
- Chugh SS, Havmoeller R, Narayanan K, Singh D, Rienstra M, Benjamin EJ, Gillum RF, Kim YH, McAnulty JH Jr, Zheng ZJ, Forouzanfar MH, Naghavi M, Mensah GA, Ezzati M, Murray CJ.. Worldwide epidemiology of atrial fibrillation: a Global Burden of Disease 2010 Study. Circulation 2014;129:837–847. - PMC - PubMed
-
- Benjamin EJ, Wolf PA, D’Agostino RB, Silbershatz H, Kannel WB, Levy D.. Impact of atrial fibrillation on the risk of death the Framingham Heart Study. Circulation 1998;98:946–952. - PubMed
-
- Kannel WB, Wolf PA, Benjamin EJ, Levy D.. Prevalence, incidence, prognosis, and predisposing conditions for atrial fibrillation: population-based estimates. Am J Cardiol 1998;82:2N–9N. - PubMed
-
- Wolf PA, Abbott RD, Kannel WB.. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke 1991;22:983–988. - PubMed
-
- Reynolds MR, Walczak J, White SA, Cohen DJ, Wilber DJ.. Improvements in symptoms and quality of life in patients with paroxysmal atrial fibrillation treated with radiofrequency catheter ablation versus antiarrhythmic drugs. Circ Cardiovasc Qual Outcomes 2010;3:615–623. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
