

Newer-Generation EGFR Inhibitors in Lung Cancer: How Are They Best Used?
- PMID: 30875928
- PMCID: PMC6468595
- DOI: 10.3390/cancers11030366
Newer-Generation EGFR Inhibitors in Lung Cancer: How Are They Best Used?
Abstract
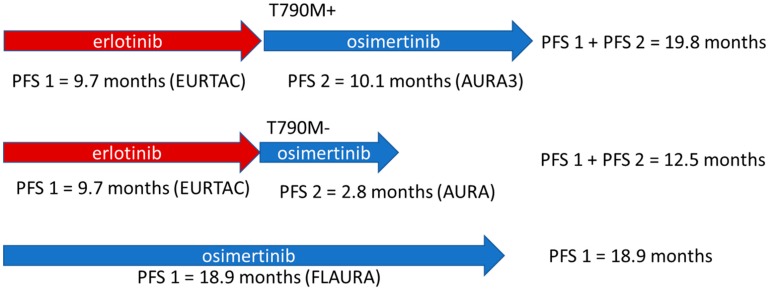
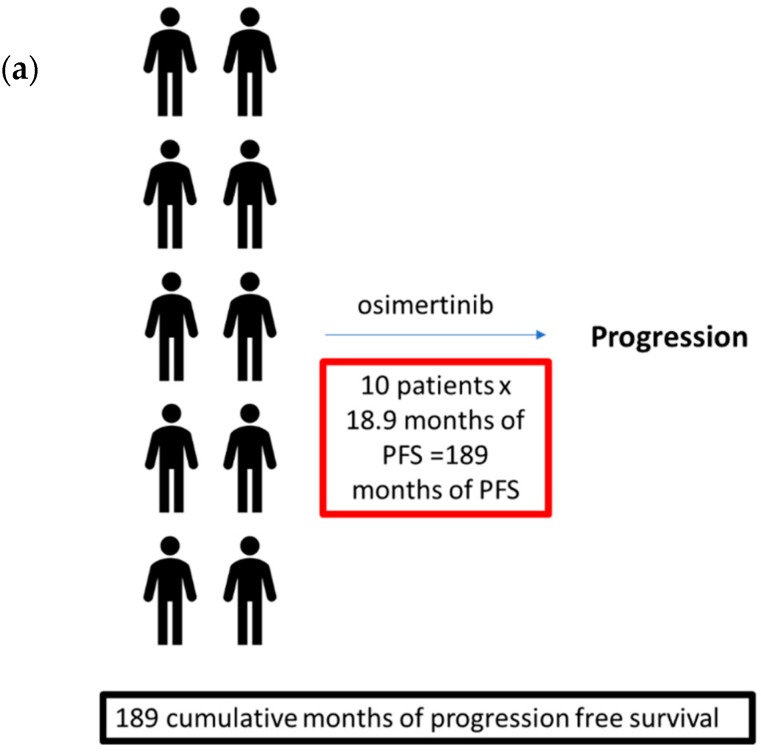
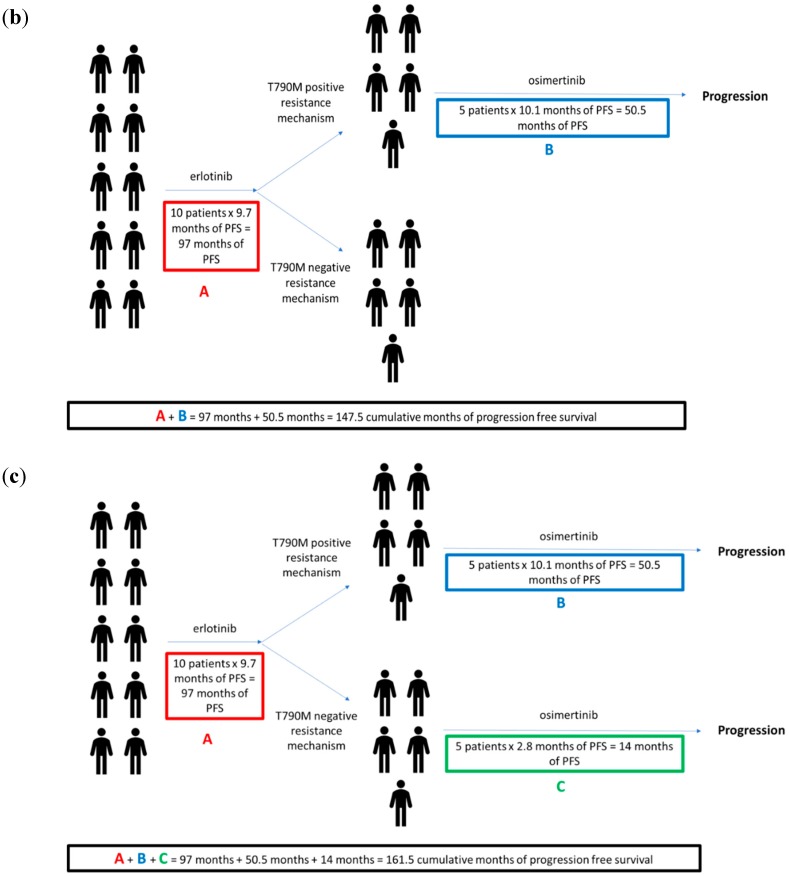
The FLAURA trial established osimertinib, a third-generation epidermal growth factor receptor (EGFR) tyrosine kinase inhibitor (TKI), as a viable first-line therapy in non-small cell lung cancer (NSCLC) with sensitizing EGFR mutations, namely exon 19 deletion and L858R. In this phase 3 randomized, controlled, double-blind trial of treatment-naïve patients with EGFR mutant NSCLC, osimertinib was compared to standard-of-care EGFR TKIs (i.e., erlotinib or gefinitib) in the first-line setting. Osimertinib demonstrated improvement in median progression-free survival (18.9 months vs. 10.2 months; hazard ratio 0.46; 95% CI, 0.37 to 0.57; p < 0.001) and a more favorable toxicity profile due to its lower affinity for wild-type EGFR. Furthermore, similar to later-generation anaplastic lymphoma kinase (ALK) inhibitors, osimertinib has improved efficacy against brain metastases. Despite this impressive effect, the optimal sequencing of osimertinib, whether in the first line or as subsequent therapy after the failure of earlier-generation EGFR TKIs, is not clear. Because up-front use of later-generation TKIs may result in the inability to use earlier-generation TKIs, this treatment paradigm must be evaluated carefully. For EGFR mutant NSCLC, considerations include the incidence of T790M resistance mutations, quality of life, whether there is a potential role for earlier-generation TKIs after osimertinib failure, and overall survival. This review explores these issues for EGFR inhibitors and other molecularly targeted therapies.
Keywords: epidermal growth factor receptor; lung cancer; osimertinib; personalized medicine; resistance; tyrosine kinase inhibitors.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Druker B.J., Guilhot F., O’Brien S.G., Gathmann I., Kantarjian H., Gattermann N., Deininger M.W., Silver R.T., Goldman J.M., Stone R.M., et al. Five-year follow-up of patients receiving imatinib for chronic myeloid leukemia. N. Engl. J. Med. 2006;355:2408–2417. doi: 10.1056/NEJMoa062867. - DOI - PubMed
-
- Guilhot F., Druker B., Larson R.A., Gathmann I., So C., Waltzman R., O’Brien S.G. High rates of durable response are achieved with imatinib after treatment with interferon alpha plus cytarabine: Results from the International Randomized Study of Interferon and STI571 (IRIS) trial. Haematologica. 2009;94:1669–1675. doi: 10.3324/haematol.2009.010629. - DOI - PMC - PubMed
-
- De Lavallade H., Apperley J.F., Khorashad J.S., Milojkovic D., Reid A.G., Bua M., Szydlo R., Olavarria E., Kaeda J., Goldman J.M., et al. Imatinib for newly diagnosed patients with chronic myeloid leukemia: Incidence of sustained responses in an intention-to-treat analysis. J. Clin. Oncol. 2008;26:3358–3363. doi: 10.1200/JCO.2007.15.8154. - DOI - PubMed
-
- Lucas C.M., Wang L., Austin G.M., Knight K., Watmough S.J., Shwe K.H., Dasgupta R., Butt N.M., Galvani D., Hoyle C.F., et al. A population study of imatinib in chronic myeloid leukaemia demonstrates lower efficacy than in clinical trials. Leukemia. 2008;22:1963–1966. doi: 10.1038/leu.2008.225. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
