

Progress in adolescent health and wellbeing: tracking 12 headline indicators for 195 countries and territories, 1990-2016
- PMID: 30876706
- PMCID: PMC6429986
- DOI: 10.1016/S0140-6736(18)32427-9
Progress in adolescent health and wellbeing: tracking 12 headline indicators for 195 countries and territories, 1990-2016
Erratum in
-
Department of Error.Lancet. 2019 Mar 23;393(10177):1204. doi: 10.1016/S0140-6736(19)30578-1. Lancet. 2019. PMID: 30910303 Free PMC article. No abstract available.
Abstract
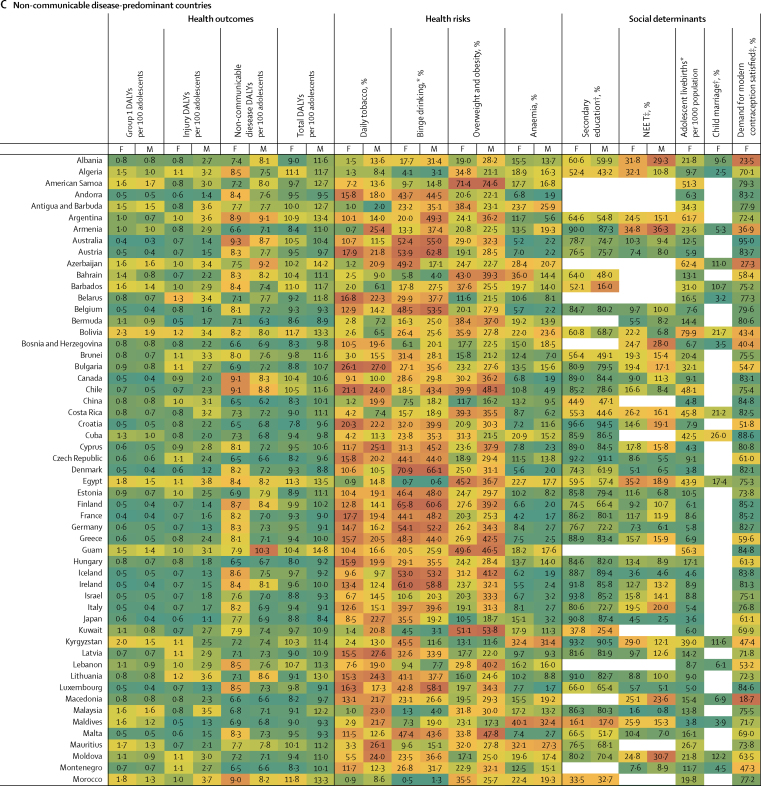
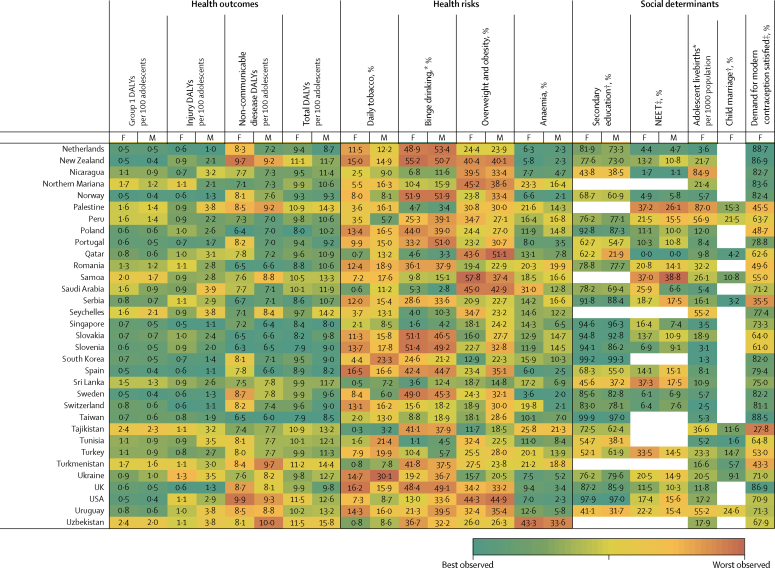
Background: Rapid demographic, epidemiological, and nutritional transitons have brought a pressing need to track progress in adolescent health. Here, we present country-level estimates of 12 headline indicators from the Lancet Commission on adolescent health and wellbeing, from 1990 to 2016.
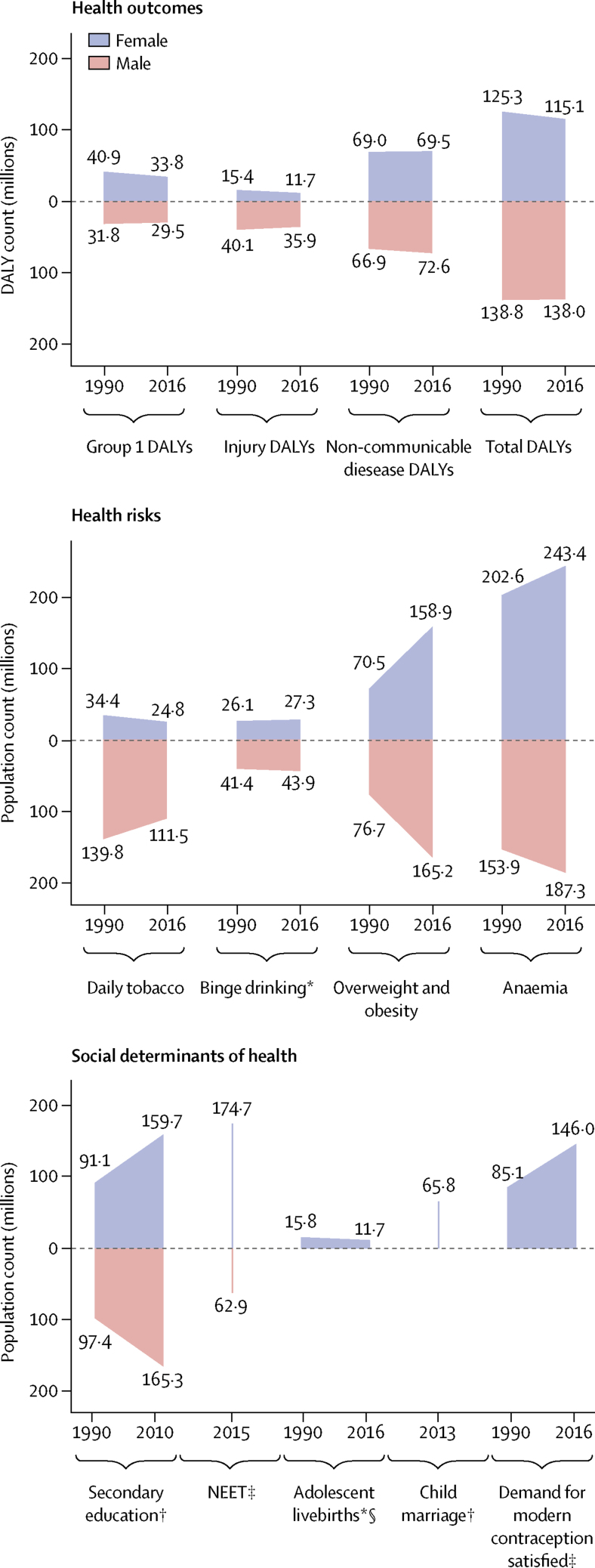
Methods: Indicators included those of health outcomes (disability-adjusted life-years [DALYs] due to communicable, maternal, and nutritional diseases; injuries; and non-communicable diseases); health risks (tobacco smoking, binge drinking, overweight, and anaemia); and social determinants of health (adolescent fertility; completion of secondary education; not in education, employment, or training [NEET]; child marriage; and demand for contraception satisfied with modern methods). We drew data from the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2016, International Labour Organisation, household surveys, and the Barro-Lee education dataset.
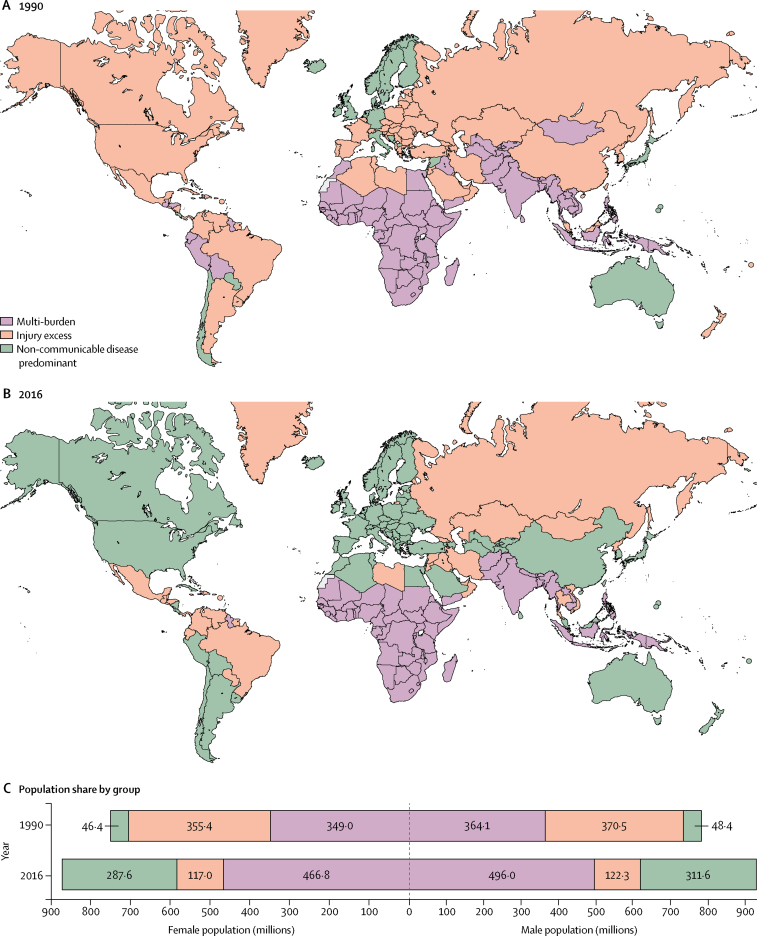
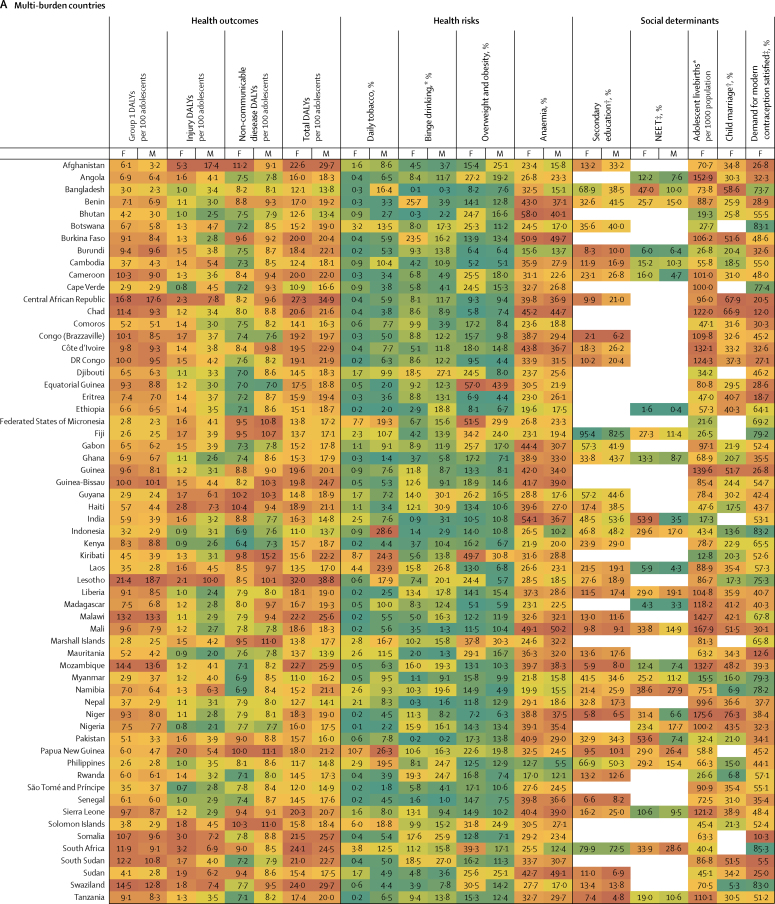
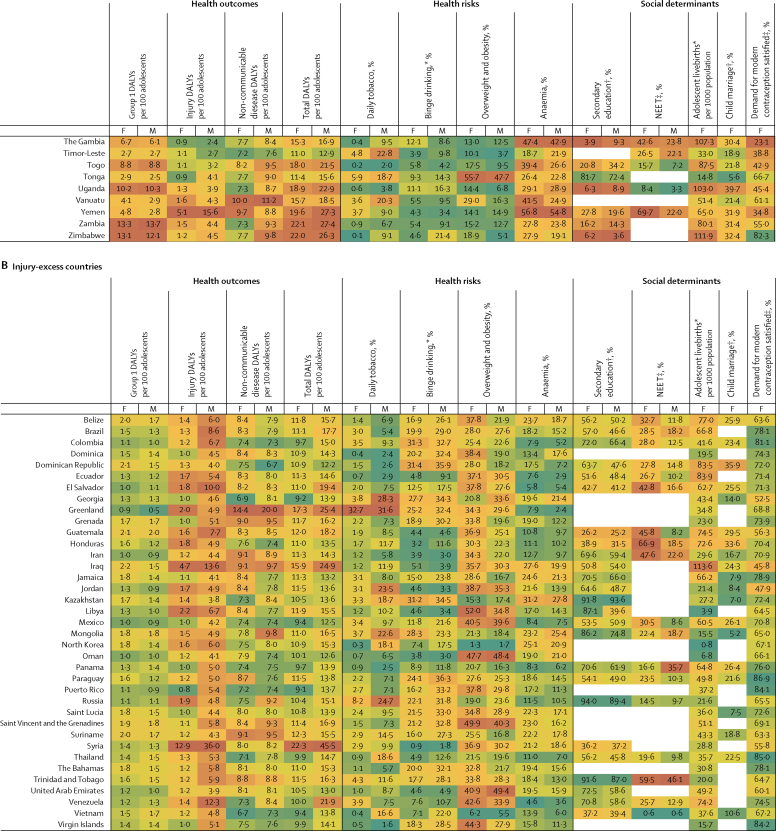
Findings: From 1990 to 2016, remarkable shifts in adolescent health occurred. A decrease in disease burden in many countries has been offset by population growth in countries with the poorest adolescent health profiles. Compared with 1990, an additional 250 million adolescents were living in multi-burden countries in 2016, where they face a heavy and complex burden of disease. The rapidity of nutritional transition is evident from the 324·1 million (18%) of 1·8 billion adolescents globally who were overweight or obese in 2016, an increase of 176·9 million compared with 1990, and the 430·7 million (24%) who had anaemia in 2016, an increase of 74·2 million compared with 1990. Child marriage remains common, with an estimated 66 million women aged 20-24 years married before age 18 years. Although gender-parity in secondary school completion exists globally, prevalence of NEET remains high for young women in multi-burden countries, suggesting few opportunities to enter the workforce in these settings.
Interpretation: Although disease burden has fallen in many settings, demographic shifts have heightened global inequalities. Global disease burden has changed little since 1990 and the prevalence of many adolescent health risks have increased. Health, education, and legal systems have not kept pace with shifting adolescent needs and demographic changes. Gender inequity remains a powerful driver of poor adolescent health in many countries.
Funding: Australian National Health and Medical Research Council, and the Bill & Melinda Gates Foundation.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Improving adolescent health: an evidence-based call to action.Lancet. 2019 Mar 16;393(10176):1073-1075. doi: 10.1016/S0140-6736(18)32996-9. Epub 2019 Mar 12. Lancet. 2019. PMID: 30876704 No abstract available.
-
Communicable diseases across the entire developmental window of childhood and adolescence: an outstanding agenda.Lancet. 2023 Jul 22;402(10398):269-271. doi: 10.1016/S0140-6736(23)01056-5. Epub 2023 Jun 29. Lancet. 2023. PMID: 37393923 No abstract available.
References
-
- Patton GC, Olsson CA, Skirbekk V. Adolescence and the next generation. Nature. 2018;554:458–466. - PubMed
-
- Sawyer S, Azzopardi P, Wickremarathne D, Patton G. The age of adolescence. Lancet Child Adolesc Health. 2018;2:223–228. - PubMed
-
- Temmerman M, Khosla R, Bhutta ZA, Bustreo F. Towards a new global strategy for women's, children's and adolescents' health. BMJ. 2015;351:h4414. - PubMed
-
- WHO . World Health Organization; Geneva: 2017. Global Accelerated Action for the Health of Adolescents (AA-HA!): guidance to support country implementation.http://apps.who.int/iris/bitstream/handle/10665/255415/9789241512343-eng...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
