

Hypertonic Saline is Superior to Mannitol for the Combined Effect on Intracranial Pressure and Cerebral Perfusion Pressure Burdens in Patients With Severe Traumatic Brain Injury
- PMID: 30877299
- PMCID: PMC8253301
- DOI: 10.1093/neuros/nyz046
Hypertonic Saline is Superior to Mannitol for the Combined Effect on Intracranial Pressure and Cerebral Perfusion Pressure Burdens in Patients With Severe Traumatic Brain Injury
Abstract
Background: Hypertonic saline (HTS) and mannitol are effective in reducing intracranial pressure (ICP) after severe traumatic brain injury (TBI). However, their simultaneous effect on the cerebral perfusion pressure (CPP) and ICP has not been studied rigorously.
Objective: To determine the difference in effects of HTS and mannitol on the combined burden of high ICP and low CPP in patients with severe TBI.
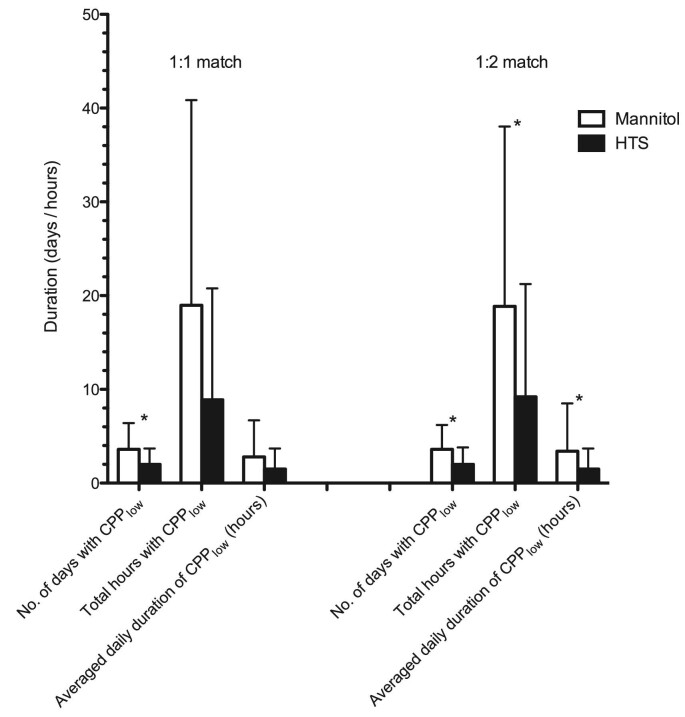
Methods: We performed a case-control study using prospectively collected data from the New York State TBI-trac® database (Brain Trauma Foundation, New York, New York). Patients who received only 1 hyperosmotic agent, either mannitol or HTS for raised ICP, were included. Patients in the 2 groups were matched (1:1 and 1:2) for factors associated with 2-wk mortality: age, Glasgow Coma Scale score, pupillary reactivity, hypotension, abnormal computed tomography scans, and craniotomy. Primary endpoint was the combined burden of ICPhigh (> 25 mm Hg) and CPPlow (< 60 mm Hg).
Results: There were 25 matched pairs for 1:1 comparison and 24 HTS patients matched to 48 mannitol patients in 1:2 comparisons. Cumulative median osmolar doses in the 2 groups were similar. In patients treated with HTS compared to mannitol, total number of days (0.6 ± 0.8 vs 2.4 ± 2.3 d, P < .01), percentage of days with (8.8 ± 10.6 vs 28.1 ± 26.9%, P < .01), and the total duration of ICPhigh + CPPlow (11.12 ± 14.11 vs 30.56 ± 31.89 h, P = .01) were significantly lower. These results were replicated in the 1:2 match comparisons.
Conclusion: HTS bolus therapy appears to be superior to mannitol in reduction of the combined burden of intracranial hypertension and associated hypoperfusion in severe TBI patients.
Keywords: Cerebral perfusion pressure; Hypertonic saline; Intracranial pressure; Mannitol; Traumatic brain injury.
Copyright © 2019 by the Congress of Neurological Surgeons.
Figures


References
-
- Langlois JA, Rutland-Brown W, Wald MM. The epidemiology and impact of traumatic brain injury. J Head Trauma Rehabil. 2006;21(5):375-378. - PubMed
-
- Gerber LM, Chiu YL, Carney N, Hartl R, Ghajar J. Marked reduction in mortality in patients with severe traumatic brain injury. J Neurosurg. 2013;119(6):1583-1590. - PubMed
-
- Bullock MR, Chesnut R, Ghajar J et al. Surgical management of acute epidural hematomas. Neurosurgery. 2006;58(3 suppl):S7-15; discussion Si-iv. - PubMed
-
- Bullock MR, Chesnut R, Ghajar J et al. Surgical management of acute subdural hematomas. Neurosurgery. 2006;58(3 Suppl):S16-24; discussion Si-iv. - PubMed
-
- Bullock MR, Chesnut R, Ghajar J et al. Surgical management of traumatic parenchymal lesions. Neurosurgery. 2006;58(3 suppl):S25-46; discussion Si-iv. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
