

Association between Non-Alcoholic Steatohepatitis and Left Ventricular Diastolic Dysfunction in Type 2 Diabetes Mellitus
- PMID: 30877708
- PMCID: PMC7188976
- DOI: 10.4093/dmj.2019.0001
Association between Non-Alcoholic Steatohepatitis and Left Ventricular Diastolic Dysfunction in Type 2 Diabetes Mellitus
Abstract
Background: Impaired diastolic heart function has been observed in persons with non-alcoholic fatty liver disease (NAFLD) and/or with type 2 diabetes mellitus (T2DM). However, it is unclear whether NAFLD fibrotic progression, i.e., non-alcoholic steatohepatitis, poses an independent risk for diastolic dysfunction in T2DM. We investigated the association between liver fibrosis and left ventricular (LV) diastolic dysfunction in T2DM.
Methods: We analyzed 606 patients with T2DM, aged ≥50 years, who had undergone liver ultrasonography and pulsed-wave Doppler echocardiography. Insulin sensitivity was measured by short insulin tolerance test. Presence of NAFLD and/or advanced liver fibrosis was determined by abdominal ultrasonography and NAFLD fibrosis score (NFS). LV diastolic dysfunction was defined according to transmitral peak early to late ventricular filling (E/A) ratio and deceleration time, using echocardiography.
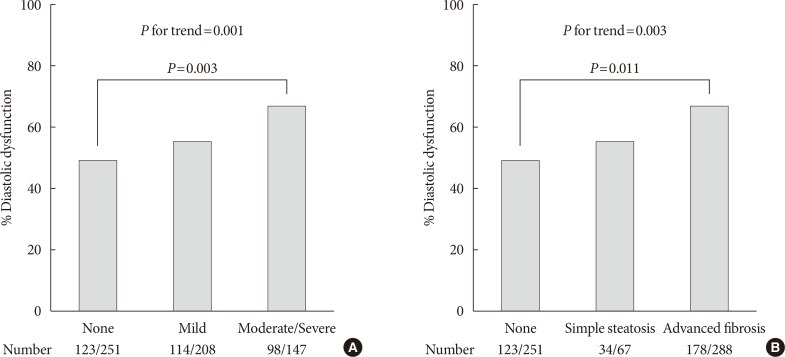
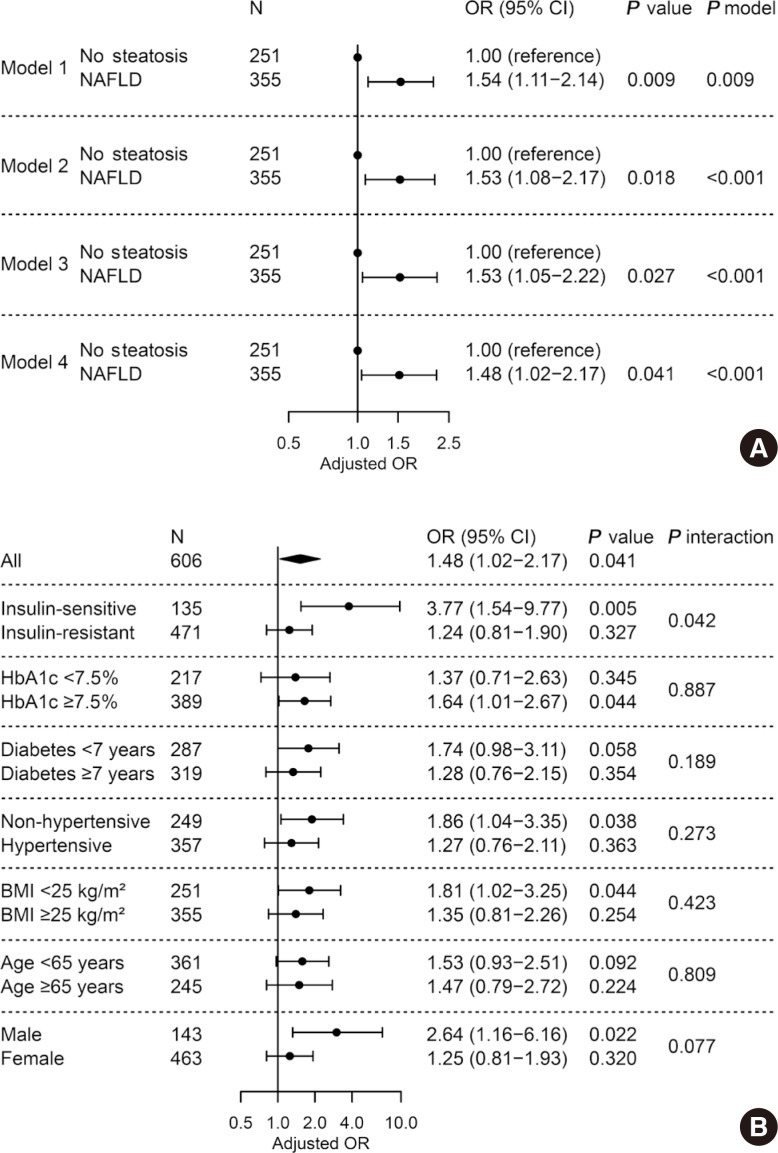
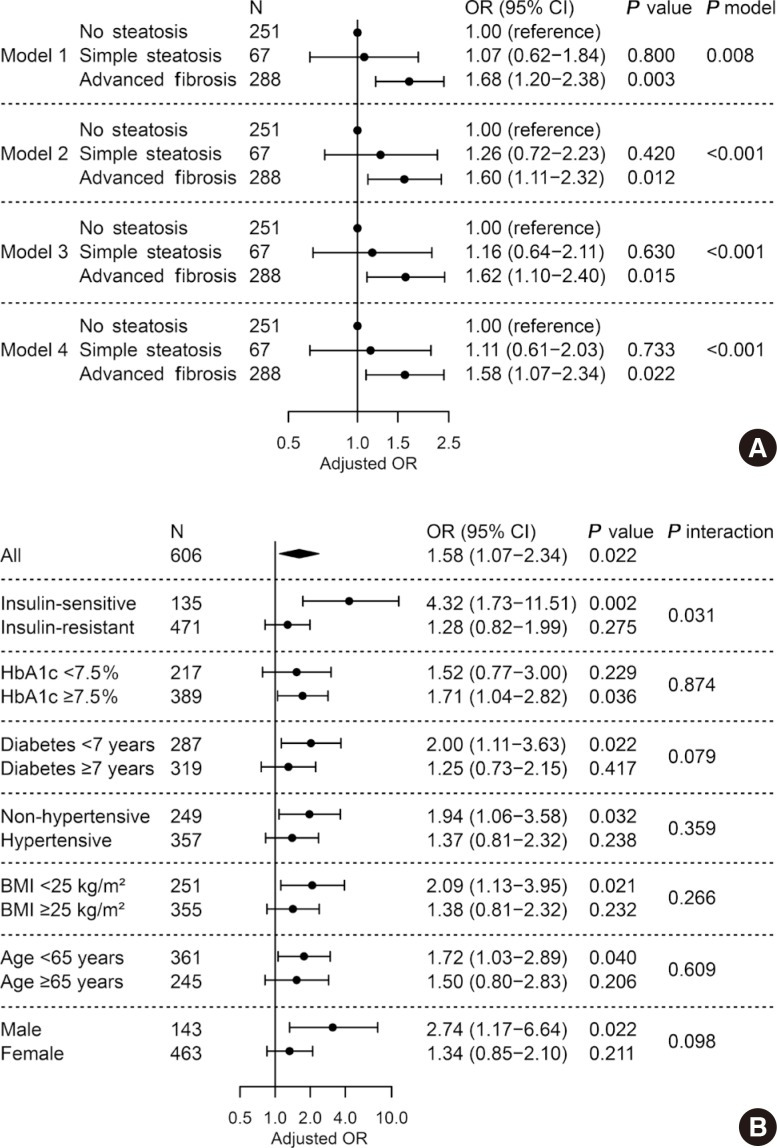
Results: LV diastolic dysfunction was significantly more prevalent in the NAFLD versus non-NAFLD group (59.7% vs. 49.0%, P=0.011). When NAFLD was stratified by NFS, subjects with advanced liver fibrosis exhibited a higher prevalence of diastolic dysfunction (49.0%, 50.7%, 61.8%; none, simple steatosis, advanced fibrosis, respectively; P for trend=0.003). In multivariable logistic regression, liver fibrosis was independently associated with diastolic dysfunction (odds ratio [OR], 1.58; 95% confidence interval [CI], 1.07 to 2.34; P=0.022) after adjusting for insulin resistance and cardiometabolic risk factors. This association remained significant in patients without insulin resistance (OR, 4.32; 95% CI, 1.73 to 11.51; P=0.002).
Conclusions: Liver fibrosis was associated with LV diastolic dysfunction in patients with T2DM and may be an independent risk factor for diastolic dysfunction, especially in patients without systemic insulin resistance.
Keywords: Diabetes mellitus, type 2; Diabetic cardiomyopathies; Heart failure; Insulin resistance; Non-alcoholic fatty liver disease.
Copyright © 2020 Korean Diabetes Association.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
Letter: Association between Non-Alcoholic Steatohepatitis and Left Ventricular Diastolic Dysfunction in Type 2 Diabetes Mellitus (Diabetes Metab J 2020;44:267-76).Diabetes Metab J. 2020 Jun;44(3):482-483. doi: 10.4093/dmj.2020.0123. Diabetes Metab J. 2020. PMID: 32613780 Free PMC article. No abstract available.
-
Response: Association between Non-Alcoholic Steatohepatitis and Left Ventricular Diastolic Dysfunction in Type 2 Diabetes Mellitus (Diabetes Metab J 2020;44:267-76).Diabetes Metab J. 2020 Jun;44(3):486-487. doi: 10.4093/dmj.2020.0127. Diabetes Metab J. 2020. PMID: 32613782 Free PMC article. No abstract available.
Similar articles
-
Nonalcoholic fatty liver disease and advanced fibrosis are associated with left ventricular diastolic dysfunction.Atherosclerosis. 2018 May;272:137-144. doi: 10.1016/j.atherosclerosis.2018.03.027. Epub 2018 Mar 17. Atherosclerosis. 2018. PMID: 29604480
-
Association of non-alcoholic steatohepatitis with subclinical myocardial dysfunction in non-cirrhotic patients.J Hepatol. 2018 Apr;68(4):764-772. doi: 10.1016/j.jhep.2017.11.023. Epub 2017 Nov 24. J Hepatol. 2018. PMID: 29175242
-
Non-alcoholic fatty liver disease is associated with left ventricular diastolic dysfunction in essential hypertension.Nutr Metab Cardiovasc Dis. 2009 Nov;19(9):646-53. doi: 10.1016/j.numecd.2008.12.007. Epub 2009 Mar 17. Nutr Metab Cardiovasc Dis. 2009. PMID: 19278843
-
Is non-alcoholic fatty liver disease a sign of left ventricular diastolic dysfunction in patients with type 2 diabetes mellitus? A systematic review and meta-analysis.BMJ Open Diabetes Res Care. 2023 Feb;11(1):e003198. doi: 10.1136/bmjdrc-2022-003198. BMJ Open Diabetes Res Care. 2023. PMID: 36807034 Free PMC article.
-
Non-Alcoholic Fatty Liver Disease in Patients with Type 2 Diabetes Mellitus: A Position Statement of the Fatty Liver Research Group of the Korean Diabetes Association.Diabetes Metab J. 2020 Jun;44(3):382-401. doi: 10.4093/dmj.2020.0010. Epub 2020 May 11. Diabetes Metab J. 2020. PMID: 32431115 Free PMC article. Review.
Cited by
-
Correlation Between 25-Hydroxyvitamin D Level and Cardiac Diastolic Dysfunction in Chinese Adults with Early-Onset Type 2 Diabetes Mellitus: A Cross-Sectional Study.Diabetes Metab Syndr Obes. 2021 Apr 28;14:1823-1831. doi: 10.2147/DMSO.S299422. eCollection 2021. Diabetes Metab Syndr Obes. 2021. PMID: 33953582 Free PMC article.
-
Assessment of left ventricular function in type 2 diabetes mellitus patients with non-alcoholic fatty liver disease using three-dimensional speckle-tracking echocardiography.Anatol J Cardiol. 2020 Jan;23(1):41-48. doi: 10.14744/AnatolJCardiol.2019.66805. Anatol J Cardiol. 2020. PMID: 31911565 Free PMC article.
-
Epidemiology of heart failure in diabetes: a disease in disguise.Diabetologia. 2024 Apr;67(4):574-601. doi: 10.1007/s00125-023-06068-2. Epub 2024 Feb 9. Diabetologia. 2024. PMID: 38334818 Free PMC article.
-
Metabolic dysfunction-associated steatotic liver disease-associated fibrosis and cardiac dysfunction in patients with type 2 diabetes.World J Cardiol. 2024 Oct 26;16(10):580-594. doi: 10.4330/wjc.v16.i10.580. World J Cardiol. 2024. PMID: 39492975 Free PMC article.
-
Interplay between Heart Disease and Metabolic Steatosis: A Contemporary Perspective.J Clin Med. 2021 Apr 8;10(8):1569. doi: 10.3390/jcm10081569. J Clin Med. 2021. PMID: 33917867 Free PMC article. Review.
References
-
- Loomba R, Sanyal AJ. The global NAFLD epidemic. Nat Rev Gastroenterol Hepatol. 2013;10:686–690. - PubMed
-
- Browning JD, Szczepaniak LS, Dobbins R, Nuremberg P, Horton JD, Cohen JC, Grundy SM, Hobbs HH. Prevalence of hepatic steatosis in an urban population in the United States: impact of ethnicity. Hepatology. 2004;40:1387–1395. - PubMed
-
- Farrell GC, Wong VW, Chitturi S. NAFLD in Asia: as common and important as in the west. Nat Rev Gastroenterol Hepatol. 2013;10:307–318. - PubMed
-
- Musso G, Cassader M, Gambino R. Non-alcoholic steatohepatitis: emerging molecular targets and therapeutic strategies. Nat Rev Drug Discov. 2016;15:249–274. - PubMed
-
- Wong RJ, Aguilar M, Cheung R, Perumpail RB, Harrison SA, Younossi ZM, Ahmed A. Nonalcoholic steatohepatitis is the second leading etiology of liver disease among adults awaiting liver transplantation in the United States. Gastroenterology. 2015;148:547–555. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
