

Changes in Mortality Involving Extended-Release and Long-Acting Opioids After Implementation of a Risk Evaluation and Mitigation Strategy
- PMID: 30877807
- PMCID: PMC6953333
- DOI: 10.1093/pm/pnz031
Changes in Mortality Involving Extended-Release and Long-Acting Opioids After Implementation of a Risk Evaluation and Mitigation Strategy
Abstract
Objective: To assess changes in mortality rates in extended-release and long-acting (ER/LA) opioid analgesics after the implementation of the Risk Evaluation and Mitigation Strategy (REMS).
Setting: All drug poisoning deaths in three states: Florida, Oregon, and Washington. Data were obtained through state vital records offices and the Researched Abuse, Diversion and Addiction-Related Surveillance System Medical Examiner Program.
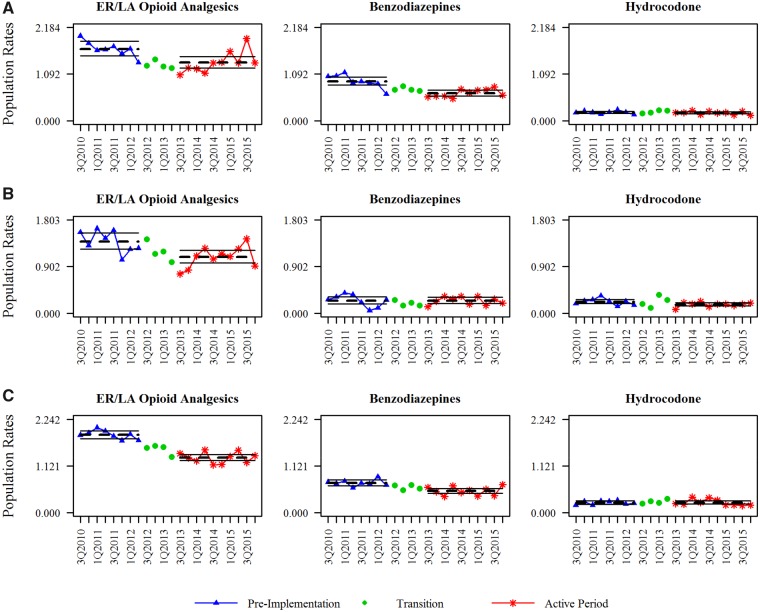
Methods: Using cause-of-death literal text from death certificates, individual opioid active pharmaceutical ingredients (APIs) involved in each death were identified using rules-based natural language processing. Population-adjusted and prescriptions dispensed-adjusted mortality rates were calculated for all ER/LA opioid analgesic and individual opioid APIs. Rates before and after implementation of the REMS were compared. Rate changes were compared with rates from two APIs with little or no inclusion in the REMS: benzodiazepines and hydrocodone.
Results: The mean ER/LA opioid analgesic population-adjusted mortality rate significantly decreased in all three states (FL: P = 0.003; OR: P = 0.003; WA: P < 0.001). Mortality rates for benzodiazepines and hydrocodone also decreased and were not statistically different. Significant heterogeneity in mortality rates of individual opioids was observed between the three states. When adjusted for prescription volume, the ER/LA opioid analgesic mortality rate decreased in all three states, but was significant only for Washington (P < 0.001).
Conclusions: The population-adjusted mortality rate of ER/LA opioid analgesics has decreased in three states. Notably, the contributions to mortality rates by individual opioid analgesics were not uniform across the three states in this study. However, these changes were not generally distinct from changes in mortality rates where comparator substances were involved.
Keywords: ER/LA; Mortality; Opioid Analgesics; Prescription Drug Abuse; REMS.
© 2019 American Academy of Pain Medicine.
Figures
Similar articles
-
Changes in misuse and abuse of prescription opioids following implementation of Extended-Release and Long-Acting Opioid Analgesic Risk Evaluation and Mitigation Strategy.Pharmacoepidemiol Drug Saf. 2017 Sep;26(9):1061-1070. doi: 10.1002/pds.4257. Epub 2017 Jul 31. Pharmacoepidemiol Drug Saf. 2017. PMID: 28758289
-
Assessing the impact of the extended-release/long-acting opioid an-algesics risk evaluation and mitigation strategies on opioid prescrip-tion volume.J Opioid Manag. 2017 May/Jun;13(3):157-168. doi: 10.5055/jom.2017.0383. J Opioid Manag. 2017. PMID: 28829517
-
ER/LA Opioid Analgesics REMS: Overview of Ongoing Assessments of Its Progress and Its Impact on Health Outcomes.Pain Med. 2017 Jan 1;18(1):78-85. doi: 10.1093/pm/pnw129. Pain Med. 2017. PMID: 27373304 Free PMC article.
-
Evaluation of the Extended-Release/Long-Acting Opioid Prescribing Risk Evaluation and Mitigation Strategy Program by the US Food and Drug Administration: A Review.JAMA Intern Med. 2020 Feb 1;180(2):301-309. doi: 10.1001/jamainternmed.2019.5459. JAMA Intern Med. 2020. PMID: 31886822 Review.
-
Evolution of opioid risk management and review of the classwide REMS for extended-release/long-acting opioids.Phys Sportsmed. 2012 Nov;40(4):12-20. doi: 10.3810/psm.2012.11.1975. Phys Sportsmed. 2012. PMID: 23306411 Review.
References
-
- Paulozzi LJ, Jones CM, Mack KA, Rudd RA.. Vital signs: Overdoses of prescription opioid pain relievers—United States, 1999–2008. MMWR Morb Mortal Wkly Rep 2011;60:1487–92. - PubMed
-
- Drug Abuse Warning Network. National Estimates of Drug-Related Emergency Department Visits. HHS Publication No. (SMA) 13-4760, DAWN Series D-39. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2013. - PubMed
-
- Centers for Disease Control and Prevention. CDC Year in Review: Working 24/7/365. Centers for Disease Control and Prevention; 2016. Available at: https://www.cdc.gov/media/dpk/cdc-24-7/eoy-2016/dpk-eoy.html (accessed April 18, 2018).
-
- Substance Abuse and Mental Health Services Administration. Treatment Episode Data Set (TEDS) 2004–2014. National Admissions to Substance Abuse Treatment Services. BHSIS Series S-84, HHS Publication No. (SMA) 16-4986. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2016.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
