

Patient and disease characteristics of type-2 diabetes patients with or without chronic kidney disease: an analysis of the German DPV and DIVE databases
- PMID: 30878037
- PMCID: PMC6420726
- DOI: 10.1186/s12933-019-0837-x
Patient and disease characteristics of type-2 diabetes patients with or without chronic kidney disease: an analysis of the German DPV and DIVE databases
Abstract
Background: To evaluate the characteristics of type 2 diabetes (T2DM) patients with or without chronic kidney disease (CKD) in Germany.
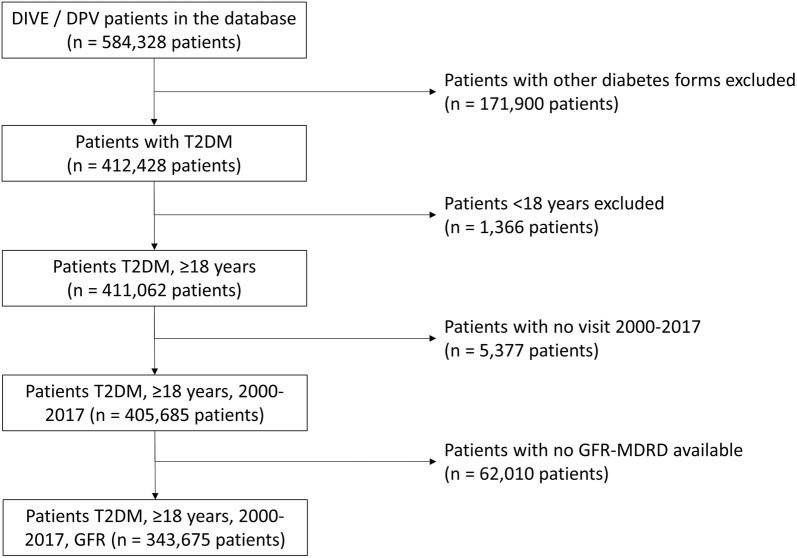
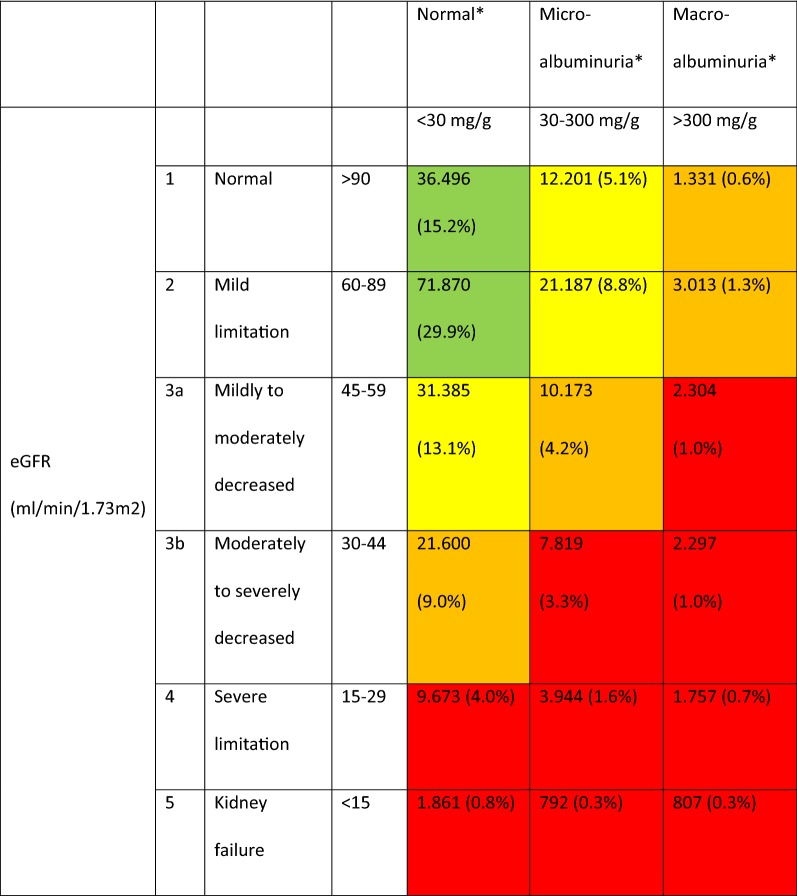
Methods: Using combined DPV/DIVE registry data, the analysis included patients with T2DM at least ≥ 18 years old who had an estimated glomerular filtration rate (eGFR) value available. CKD was defined as an eGFR < 60 mL/min/1.73 m2 or eGFR ≥ 60 mL/min/1.73 m2 and albuminuria (≥ 30 mg/g). Median values of the most recent treatment year per patient are reported.
Results: Among 343,675 patients with T2DM 171,930 had CKD. Patients with CKD had a median eGFR of 48.9 mL/min/1.73 m2 and 51.2% had a urinary albumin level ≥ 30 mg/g. They were older, had a longer diabetes duration and a higher proportion was females compared to patients without CKD (all p < 0.001). More than half of CKD patients (53.5%) were receiving long-acting insulin-based therapy versus around 39.1% of those without (p < 0.001). CKD patients also had a higher rate of hypertension (79.4% vs 72.0%; p < 0.001). The most common antihypertensive drugs among CKD patients were renin-angiotensin-aldosteron system inhibitors (angiotensin converting enzyme inhibitors 33.8%, angiotensin receptor blockers 14.2%) and diuretics (40.2%). CKD patients had a higher rate of dyslipidemia (88.4% vs 86.3%) with higher triglyceride levels (157.9 vs 151.0 mg/dL) and lower HDL-C levels (men: 40.0 vs 42.0 mg/dL; women: 46.4 vs 50.0 mg/dL) (all p < 0.001) and a higher rate of hyperkalemia (> 5.5 mmol/L: 3.7% vs. 1.0%). Comorbidities were more common among CKD patients (p < 0.001).
Conclusion: The results illustrate the prevalence and morbidity burden associated with diabetic kidney disease in patients with T2DM in Germany. The data call for more attention to the presence of chronic kidney disease in patients with diabetes, should trigger intensified risk factor control up and beyond the control of blood glucose and HbA1c in these patients. They may also serve as a trigger for future investigations into this patient population asking for new treatment options to be developed.
Keywords: Chronic kidney disease; DIVE; DPV; Disease characteristics; Patient characteristics; Type-2-diabetes.
Conflict of interest statement
JS and TD report grants and personal fees from Abbott, AstraZeneca, and Sanofi, outside the submitted work. PB reports to have received consultancy honoraria from Sanofi and Abbott. SL, GvM, EH, SF, CHJH, MF, and RWH declares that they have no competing interests.
Figures
References
-
- Xie Y, Bowe B, Mokdad AH, Xian H, Yan Y, Li T, Maddukuri G, Tsai CY, Floyd T, Al-Aly Z. Analysis of the global burden of disease study highlights the global, regional, and national trends of chronic kidney disease epidemiology from 1990 to 2016. Kidney Int. 2018;94(3):567–581. doi: 10.1016/j.kint.2018.04.011. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
