

Efficacy and risk of harms of repeat ivermectin mass drug administrations for control of malaria (RIMDAMAL): a cluster-randomised trial
- PMID: 30878222
- PMCID: PMC6459982
- DOI: 10.1016/S0140-6736(18)32321-3
Efficacy and risk of harms of repeat ivermectin mass drug administrations for control of malaria (RIMDAMAL): a cluster-randomised trial
Abstract
Background: Ivermectin is widely used in mass drug administrations for controlling neglected parasitic diseases, and can be lethal to malaria vectors that bite treated humans. Therefore, it could be a new tool to reduce plasmodium transmission. We tested the hypothesis that frequently repeated mass administrations of ivermectin to village residents would reduce clinical malaria episodes in children and would be well tolerated with minimal harms.
Methods: We invited villages (clusters) in Burkina Faso to participate in a single-blind (outcomes assessor), parallel-assignment, two-arm, cluster-randomised trial over the 2015 rainy season. Villages were assigned (1:1) by random draw to either the intervention group or the control group. In both groups, all eligible participants who consented to the treatment and were at least 90 cm in height received single oral doses of ivermectin (150-200 μg/kg) and albendazole (400 mg), and those in the intervention group received five further doses of ivermectin alone at 3-week intervals thereafter over the 18-week treatment phase. The primary outcome was cumulative incidence of uncomplicated malaria episodes over 18 weeks (analysed on a cluster intention-to-treat basis) in an active case detection cohort of children aged 5 years or younger living in the study villages. This trial is registered with ClinicalTrials.gov, number NCT02509481.
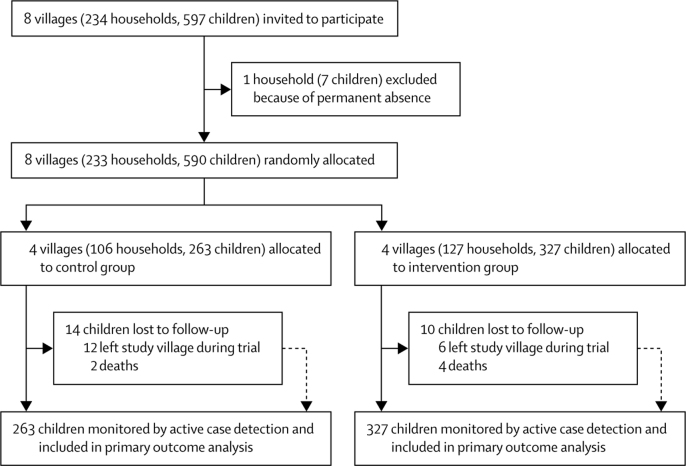
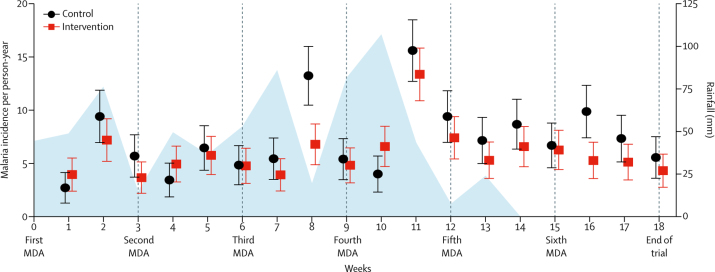
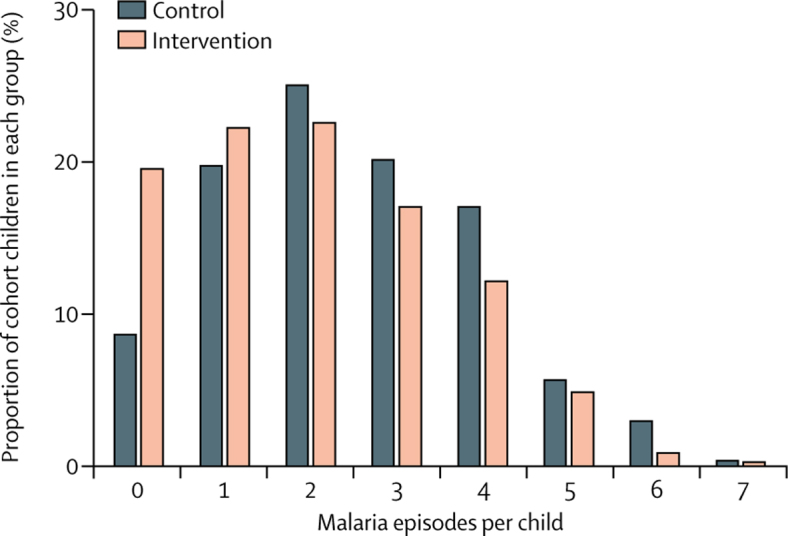
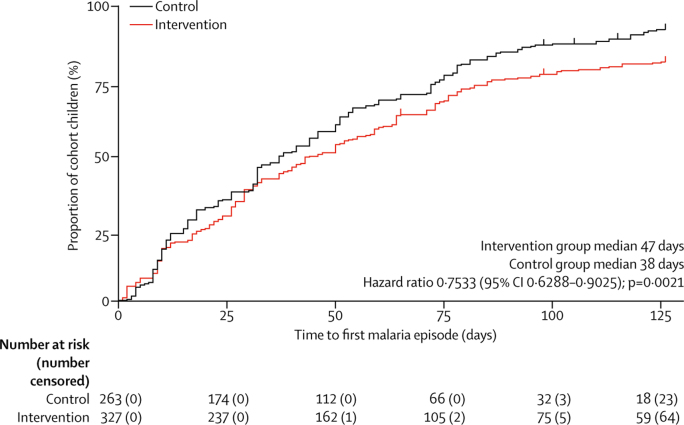
Findings: Eight villages agreed to participate, and four were randomly assigned to each group. 2712 participants (1333 [49%] males and 1379 [51%] females; median age 15 years [IQR 6-34]), including 590 children aged 5 years or younger, provided consent and were enrolled between May 22 and July 20, 2015 (except for 77 participants enrolled after these dates because of unavailability before the first mass drug administration, travel into the village during the trial, or birth), with 1447 enrolled into the intervention group and 1265 into the control group. 330 (23%) participants in the intervention group and 233 (18%) in the control group met the exclusion criteria for mass drug administration. Most children in the active case detection cohort were not treated because of height restrictions. 14 (4%) children in the intervention group and 10 (4%) in the control group were lost to follow-up. Cumulative malaria incidence was reduced in the intervention group (648 episodes among 327 children; estimated mean 2·00 episodes per child) compared with the control group (647 episodes among 263 children; 2·49 episodes per child; risk difference -0·49 [95% CI -0·79 to -0·21], p=0·0009, adjusted for sex and clustering). The risk of adverse events among all participants did not differ between groups (45 events [3%] among 1447 participants in the intervention group vs 24 events [2%] among 1265 in the control group; risk ratio 1·63 [1·01 to 2·67]; risk difference 1·21 [0·04 to 2·38], p=0·060), and no adverse reactions were reported.
Interpretation: Frequently repeated mass administrations of ivermectin during the malaria transmission season can reduce malaria episodes among children without significantly increasing harms in the populace.
Funding: Bill & Melinda Gates Foundation.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Advancing the repurposing of ivermectin for malaria.Lancet. 2019 Apr 13;393(10180):1480-1481. doi: 10.1016/S0140-6736(18)32613-8. Epub 2019 Mar 14. Lancet. 2019. PMID: 30878223 No abstract available.
-
Analysis of the RIMDAMAL trial.Lancet. 2019 Sep 21;394(10203):1005-1006. doi: 10.1016/S0140-6736(19)31663-0. Epub 2019 Jul 16. Lancet. 2019. PMID: 31324344 No abstract available.
-
Analysis of the RIMDAMAL trial.Lancet. 2019 Sep 21;394(10203):1006. doi: 10.1016/S0140-6736(19)31814-8. Lancet. 2019. PMID: 31544741 No abstract available.
-
Analysis of the RIMDAMAL trial - Authors' reply.Lancet. 2019 Sep 21;394(10203):1006-1007. doi: 10.1016/S0140-6736(19)32139-7. Lancet. 2019. PMID: 31544742 No abstract available.
References
-
- WHO . World Health Organization; Geneva: 2017. World malaria report 2017; p. 160.
-
- Dondorp AM, Yeung S, White L. Artemisinin resistance: current status and scenarios for containment. Nat Rev Microbiol. 2010;8:272–280. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
