

Effect of increased dose of total body irradiation on graft failure associated with HLA-haploidentical transplantation in patients with severe haemoglobinopathies: a prospective clinical trial
- PMID: 30878319
- PMCID: PMC6506220
- DOI: 10.1016/S2352-3026(19)30031-6
Effect of increased dose of total body irradiation on graft failure associated with HLA-haploidentical transplantation in patients with severe haemoglobinopathies: a prospective clinical trial
Erratum in
-
Correction to Lancet Haematol 2019; 6: e183-93.Lancet Haematol. 2019 May;6(5):e238. doi: 10.1016/S2352-3026(19)30067-5. Lancet Haematol. 2019. PMID: 31036316 No abstract available.
Abstract
Background: Although severe haemoglobinopathies can be cured with allogeneic blood or bone marrow transplantation, availability of matched donors and toxic effects can be problematic. We previously found that non-myeloablative haploidentical related bone marrow transplantation with post-transplantation cyclophosphamide expanded the donor pool while limiting graft-versus-host disease (GVHD). However, graft failure-albeit with full host haemopoietic recovery-occurred in 50% of patients. In this study, we investigated whether increasing total body irradiation from 200 cGy to 400 cGy would improve engraftment while maintaining the safety profile.
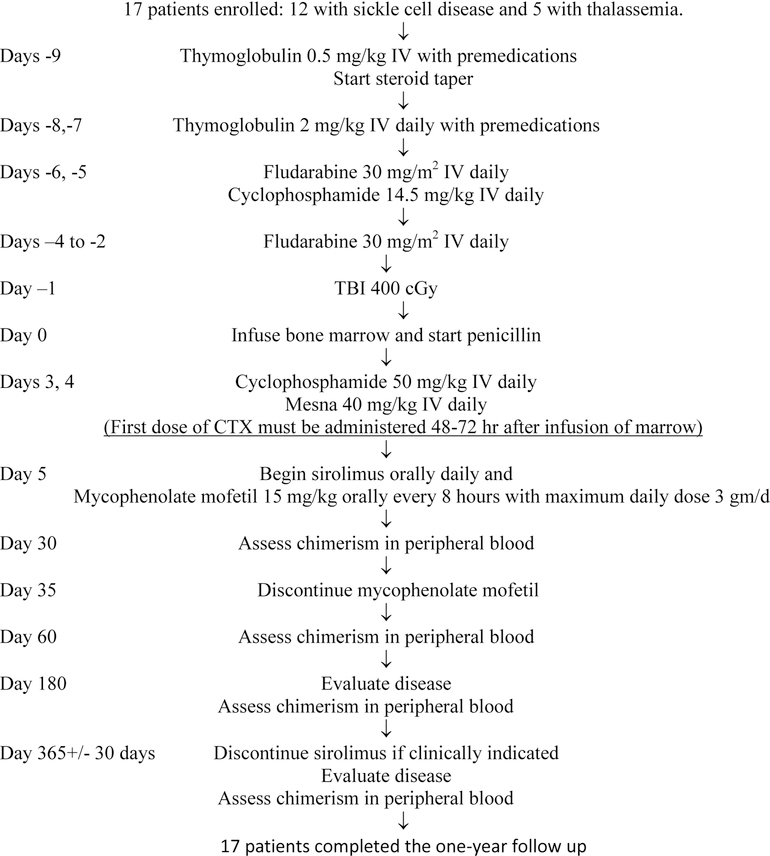
Methods: This study was done at Johns Hopkins Hospital (Baltimore, MD, USA). Patients aged 2-70 years receiving their first bone marrow transplant were eligible for inclusion in the study. Patients received rabbit-derived intravenous anti-thymocyte globulin 0·5 mg/kg on day -9 and 2 mg/kg on days -8 and -7, intravenous fludarabine 30 mg/m2 on days -6 to -2, intravenous cyclophosphamide 14·5 mg/kg on days -6 and -5, and total body irradiation 400 cGy administered as a single fraction on day -1. We collected unmanipulated bone marrow and infused on day 0. GVHD prophylaxis comprised intravenous cyclophosphamide 50 mg/kg per day on days 3 and 4 after transplantation, oral mycophenolate mofetil 15 mg/kg per dose (maximum 1 g) every 8 h on days 5 to 35, and oral sirolimus to maintain a level of 5-15 ng/dL for at least 1 year starting on day 5. The original planned primary objectives of this phase 2 clinical trial were transplant-related mortality and progression-free survival. However, the coverage decision by the Centers for Medicare and Medicaid Services to only provide payment for allogeneic bone marrow transplantation for patients with sickle cell disease on a clinical trial that had a comparison arm with patients not receiving bone marrow transplantation prompted the closure of this trial to accrual in 2017. Therefore, as we were unable to perform our planned statistical analysis, the primary objective was modified to evaluate engraftment, assessed by chimerism. This trial is registered with ClinicalTrials.gov, number NCT00489281. The study is closed to new participants and this is the primary analysis.
Findings: Between Sept 24, 2014, and Aug 1, 2017, we enrolled 17 consecutive patients: 12 (71%) with sickle cell disease and 5 (29%) with β-thalassaemia major. The median patient age was 16 years (range 6-31, IQR 7·7-27·5). One (6%) of 17 patients had primary graft failure with recovery of host haemopoiesis. 13 (76%) of 17 patients achieved full donor chimerism and three (18%) had mixed donor-host chimerism. Five (29%) of 17 patients developed grade 2-4 acute GVHD, including four (24%) with maximal grade 2 GVHD and one (6%) with grade 3 GVHD. Chronic GVHD developed in three (18%) patients. As of their last follow-up visit, GVHD had resolved in all patients and no patients were receiving systemic GVHD therapy. All patients remained alive as of Aug 4, 2019, and the median follow-up duration was 705 days (range 355-1294; IQR 398-943). Only one (6%) of the 16 engrafted patients remained transfusion dependent, and 14 (88%) discontinued immunosuppression.
Interpretation: Increasing total body irradiation to 400 cGy substantially reduced graft failure while maintaining the safety of haploidentical bone marrow transplantation with post-transplantation cyclophosphamide. These results suggest that engraftment after haploidentical bone marrow transplantation for haemoglobinopathies is possible, and primary graft failure-the main problem previously reported-might be addressed by this strategy. Therefore, this curative approach should no longer be restricted to patients with HLA-matched donors.
Funding: Maryland Stem Cell Research Fund and US National Institutes of Health.
Copyright © 2019 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Conflict of Interest Disclosures:
Dr. Ali reports consulting and research funding from Celgene, consulting, Advisory Board, research funding from Aduro Biotech, Advisory Board from Bristol Myers-Squibb, Advisory Board from Amgen, Advisory Board from Takeda, outside the submitted work.
Dr. Bolaños-Meade reports DSMB fees from Incyte Corporation, outside the submitted work.
Dr. Brodsky reports grants from Maryland State Stem Cell Fund/TEDCO, during the conduct of the study; Scientific Advisory Board and research funding from Alexion Pharmaceutical, and Achillion Pharmaceutical, outside the submitted work.
Dr. Cooke reports grants from MSCRF, grants from NIH, during the conduct of the study
Dr. Luznik reports Advisory Board fees from AbbVie, speaking engagement from Merck, grants from Gennentech, Advisory Board fees from Pharamacyclics.
Dr. Symons reports belonging to the Speaker’s Bureau for Jazz pharmaceuticals re: Defetilio. she helped create the slideset, speak about veno-occlussive disease pathophysiology as well as treatment. Dr. Terezakis reports a scientific grant from ASELL and a scientific grant from Elekta Industries, outside the submitted work.
Dr. Wagner-Johnston reports other from Advisory Board fees from Gilead, other from Bayer, other from JUNO, other from ADC Therapeutics, other from Janssen, outside the submitted work.
The other authors declared no conflict of interest.
Comment in
-
Improvements in haploidentical transplantation for sickle cell disease and β-thalassaemia.Lancet Haematol. 2019 Apr;6(4):e168-e169. doi: 10.1016/S2352-3026(19)30045-6. Epub 2019 Mar 14. Lancet Haematol. 2019. PMID: 30878318 No abstract available.
Similar articles
-
Haploidentical bone marrow transplantation in patients with relapsed or refractory severe aplastic anaemia in the USA (BMT CTN 1502): a multicentre, single-arm, phase 2 trial.Lancet Haematol. 2022 Sep;9(9):e660-e669. doi: 10.1016/S2352-3026(22)00206-X. Epub 2022 Jul 27. Lancet Haematol. 2022. PMID: 35907408 Free PMC article. Clinical Trial.
-
Addition of sirolimus to standard cyclosporine plus mycophenolate mofetil-based graft-versus-host disease prophylaxis for patients after unrelated non-myeloablative haemopoietic stem cell transplantation: a multicentre, randomised, phase 3 trial.Lancet Haematol. 2019 Aug;6(8):e409-e418. doi: 10.1016/S2352-3026(19)30088-2. Epub 2019 Jun 24. Lancet Haematol. 2019. PMID: 31248843 Free PMC article. Clinical Trial.
-
Hematopoietic stem cell transplantation using single UM171-expanded cord blood: a single-arm, phase 1-2 safety and feasibility study.Lancet Haematol. 2020 Feb;7(2):e134-e145. doi: 10.1016/S2352-3026(19)30202-9. Epub 2019 Nov 6. Lancet Haematol. 2020. PMID: 31704264 Clinical Trial.
-
Allogeneic Blood or Marrow Transplantation with Post-Transplantation Cyclophosphamide for Peripheral T Cell Lymphoma: The Importance of Graft Source.Transplant Cell Ther. 2023 Apr;29(4):267.e1-267.e5. doi: 10.1016/j.jtct.2022.12.009. Epub 2022 Dec 19. Transplant Cell Ther. 2023. PMID: 36549386 Free PMC article. Review.
-
Alloreactivity as therapeutic principle in the treatment of hematologic malignancies. Studies of clinical and immunologic aspects of allogeneic hematopoietic cell transplantation with nonmyeloablative conditioning.Dan Med Bull. 2007 May;54(2):112-39. Dan Med Bull. 2007. PMID: 17521527 Review.
Cited by
-
Genetic therapies for the first molecular disease.J Clin Invest. 2021 Apr 15;131(8):e146394. doi: 10.1172/JCI146394. J Clin Invest. 2021. PMID: 33855970 Free PMC article. Review.
-
Organ function indications and potential improvements following curative therapy for sickle cell disease.Hematology Am Soc Hematol Educ Program. 2022 Dec 9;2022(1):277-282. doi: 10.1182/hematology.2022000372. Hematology Am Soc Hematol Educ Program. 2022. PMID: 36485131 Free PMC article.
-
Controversies and expectations for the prevention of GVHD: A biological and clinical perspective.Front Immunol. 2022 Nov 23;13:1057694. doi: 10.3389/fimmu.2022.1057694. eCollection 2022. Front Immunol. 2022. PMID: 36505500 Free PMC article. Review.
-
Guidelines on sickle cell disease: secondary stroke prevention in children and adolescents. Associação Brasileira de Hematologia, Hemoterapia e Terapia Celular guidelines project: Associação Médica Brasileira - 2022.Hematol Transfus Cell Ther. 2022 Apr-Jun;44(2):246-255. doi: 10.1016/j.htct.2022.01.010. Epub 2022 Feb 25. Hematol Transfus Cell Ther. 2022. PMID: 35305940 Free PMC article. No abstract available.
-
Sickle Cell Transplantation Evaluation of Long-term and Late Effects Registry (STELLAR) to Compare Long-term Outcomes After Hematopoietic Cell Transplantation to Those in Siblings Without Sickle Cell Disease and in Nontransplanted Individuals With Sickle Cell Disease: Design and Feasibility Study.JMIR Res Protoc. 2022 Jul 6;11(7):e36780. doi: 10.2196/36780. JMIR Res Protoc. 2022. PMID: 35793124 Free PMC article.
References
-
- Lorey FW, Arnopp J, Cunningham GC. Distribution of hemoglobinopathy variants by ethnicity in a multiethnic state. Genet Epidemiol 1996;13(5):501–12. - PubMed
-
- Kauf TL, Coates TD, Huazhi L, Mody-Patel N, Hartzema AG. The cost of health care for children and adults with sickle cell disease. Am J Hematol 2009;84(6):323–7. - PubMed
-
- Ballas SK, Bauserman RL, McCarthy WF, Waclawiw MA. The impact of hydroxyurea on career and employment of patients with sickle cell anemia. J Natl Med Assoc 2010;102(11):993–9. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
