

Epidemiology of Shock in Contemporary Cardiac Intensive Care Units
- PMID: 30879324
- PMCID: PMC11032172
- DOI: 10.1161/CIRCOUTCOMES.119.005618
Epidemiology of Shock in Contemporary Cardiac Intensive Care Units
Abstract
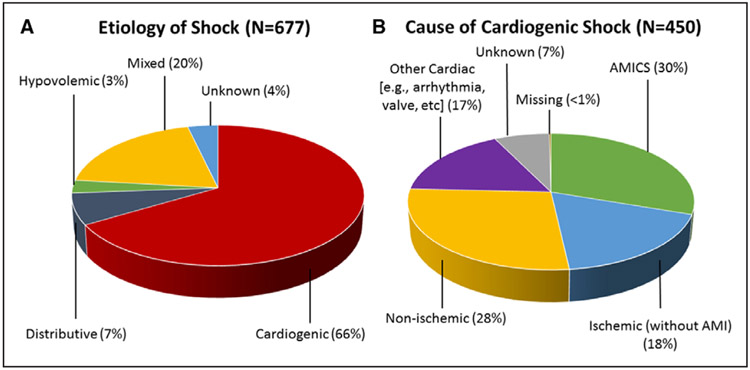
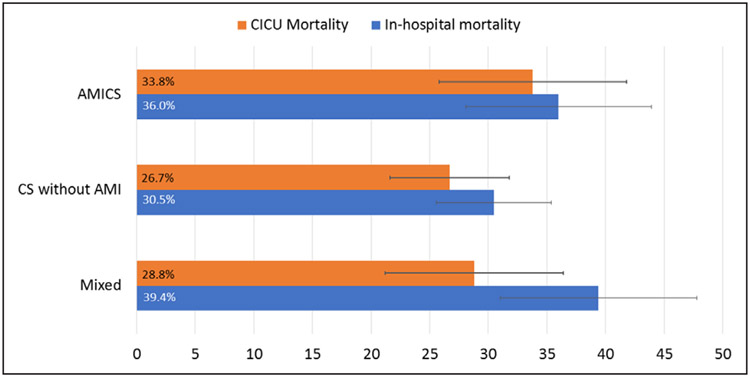
Background Clinical investigations of shock in cardiac intensive care units (CICUs) have primarily focused on acute myocardial infarction (AMI) complicated by cardiogenic shock (AMICS). Few studies have evaluated the full spectrum of shock in contemporary CICUs. Methods and Results The Critical Care Cardiology Trials Network is a multicenter network of advanced CICUs in North America. Anytime between September 2017 and September 2018, each center (n=16) contributed a 2-month snap-shot of all consecutive medical admissions to the CICU. Data were submitted to the central coordinating center (TIMI Study Group, Boston, MA). Shock was defined as sustained systolic blood pressure <90 mm Hg with end-organ dysfunction ascribed to the hypotension. Shock type was classified by site investigators as cardiogenic, distributive, hypovolemic, or mixed. Among 3049 CICU admissions, 677 (22%) met clinical criteria for shock. Shock type was varied, with 66% assessed as cardiogenic shock (CS), 7% as distributive, 3% as hypovolemic, 20% as mixed, and 4% as unknown. Among patients with CS (n=450), 30% had AMICS, 18% had ischemic cardiomyopathy without AMI, 28% had nonischemic cardiomyopathy, and 17% had a cardiac cause other than primary myocardial dysfunction. Patients with mixed shock had cardiovascular comorbidities similar to patients with CS. The median CICU stay was 4.0 days (interquartile range [IQR], 2.5-8.1 days) for AMICS, 4.3 days (IQR, 2.1-8.5 days) for CS not related to AMI, and 5.8 days (IQR, 2.9-10.0 days) for mixed shock versus 1.9 days (IQR, 1.0-3.6) for patients without shock ( P<0.01 for each). Median Sequential Organ Failure Assessment scores were higher in patients with mixed shock (10; IQR, 6-13) versus AMICS (8; IQR, 5-11) or CS without AMI (7; IQR, 5-11; each P<0.01). In-hospital mortality rates were 36% (95% CI, 28%-45%), 31% (95% CI, 26%-36%), and 39% (95% CI, 31%-48%) in AMICS, CS without AMI, and mixed shock, respectively. Conclusions The epidemiology of shock in contemporary advanced CICUs is varied, and AMICS now represents less than one-third of all CS. Despite advanced therapies, mortality in CS and mixed shock remains high. Investigation of management strategies and new therapies to treat shock in the CICU should take this epidemiology into account.
Keywords: North America; cardiogenic shock; epidemiology; hypotension; intensive care units.
Figures
References
-
- Hochman JS, Sleeper LA, Webb JG, Sanborn TA, White HD, Talley JD, Buller CE, Jacobs AK, Slater JN, Col J, McKinlay SM, LeJemtel TH. Early revascularization in acute myocardial infarction complicated by cardiogenic shock. SHOCK Investigators. Should we emergently revascularize occluded coronaries for cardiogenic shock. N Engl J Med. 1999;341:625–634. doi: 10.1056/NEJM199908263410901 - DOI - PubMed
-
- Goldberg RJ, Spencer FA, Gore JM, Lessard D, Yarzebski J. Thirty-year trends (1975 to 2005) in the magnitude of, management of, and hospital death rates associated with cardiogenic shock in patients with acute myocardial infarction: a population-based perspective. Circulation. 2009;119:1211–1219. doi: 10.1161/CIRCULATIONAHA.108.814947 - DOI - PMC - PubMed
-
- Aissaoui N, Puymirat E, Tabone X, Charbonnier B, Schiele F, Lefèvre T, Durand E, Blanchard D, Simon T, Cambou JP, Danchin N. Improved outcome of cardiogenic shock at the acute stage of myocardial infarction: a report from the USIK 1995, USIC 2000, and FAST-MI French nationwide registries. Eur Heart J. 2012;33:2535–2543. doi: 10.1093/eurheartj/ehs264 - DOI - PubMed
-
- Kolte D, Khera S, Aronow WS, Mujib M, Palaniswamy C, Sule S, Jain D, Gotsis W, Ahmed A, Frishman WH, Fonarow GC. Trends in incidence, management, and outcomes of cardiogenic shock complicating ST-elevation myocardial infarction in the United States. J Am Heart Assoc. 2014;3:e000590. doi: 10.1161/JAHA.113.000590 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
