

Telemedicine in Prehospital Acute Stroke Care
- PMID: 30879372
- PMCID: PMC6475065
- DOI: 10.1161/JAHA.118.011729
Telemedicine in Prehospital Acute Stroke Care
Abstract
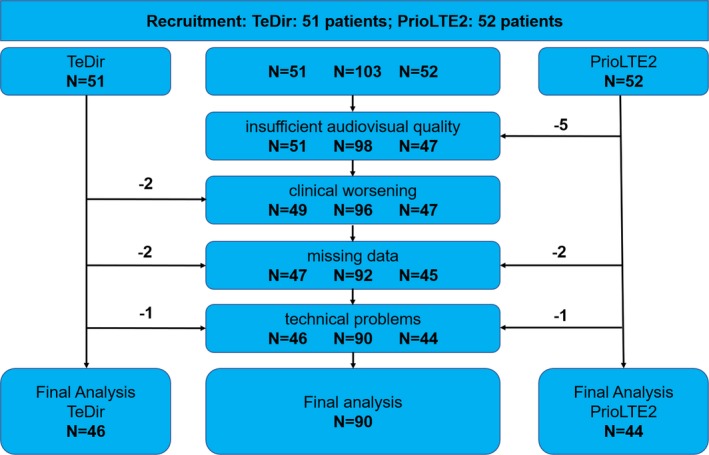
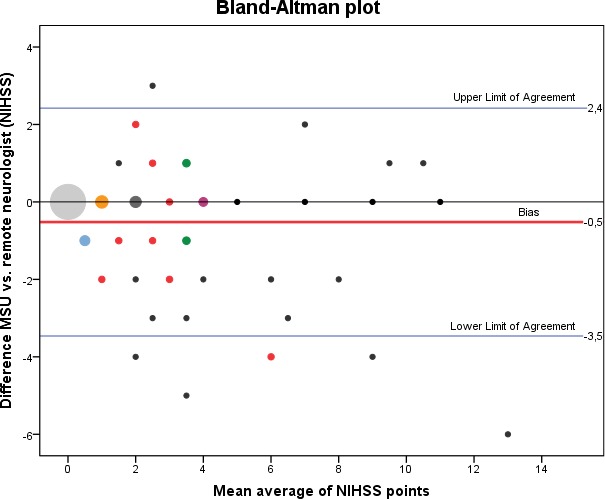
Background Mobile stroke units ( MSU s), equipped with an integrated computed tomography scanner, can shorten time to thrombolytic treatment and may improve outcome in patients with acute ischemic stroke. Original (German) MSU s are staffed by neurologists trained as emergency physicians, but patient assessment and treatment decisions by a remote neurologist may offer an alternative to neurologists aboard MSU . Methods and Results Remote neurologists examined and assessed emergency patients treated aboard the MSU in Berlin, Germany. Audiovisual quality was rated by the remote neurologist from 1 (excellent) to 6 (insufficient), and duration of video examinations was assessed. We analyzed interrater reliability of diagnoses, scores on the National Institutes of Health Stroke Scale and treatment decisions (intravenous thrombolysis) between the MSU neurologist and the remote neurologist. We included 90 of 103 emergency assessments (13 patients were excluded because of either failed connection, technical problems, clinical worsening during teleconsultation, or missing data in documentation) in this study. The remote neurologist rated audiovisual quality with a median grade for audio quality of 3 (satisfactory) and for video quality of 2 (good). Mean time for completion of teleconsultations was about 19±5 minutes. The interrater reliabilities between the onboard and remote neurologist were high for diagnoses (Cohen's κ=0.86), National Institutes of Health Stroke Scale sum scores (intraclass correlation coefficient, 0.87) and treatment decisions (16 treatment decisions agreed versus 2 disagreed; Cohen's κ=0.93). Conclusions Remote assessment and treatment decisions of emergency patients are technically feasible with satisfactory audiovisual quality. Agreement on diagnoses, neurological examinations, and treatment decisions between onboard and remote neurologists was high.
Keywords: emergency medical services; emergency medicine; ischemic stroke; telemedicine; thrombolysis.
Figures
Comment in
-
Telemedicine in Prehospital Acute Stroke Care: An Expanding Infrastructure for Treatment and Research.J Am Heart Assoc. 2019 Mar 19;8(6):e012259. doi: 10.1161/JAHA.119.012259. J Am Heart Assoc. 2019. PMID: 30879369 Free PMC article.
References
-
- Lees KR, Bluhmki E, vonKummer R , Brott TG, Toni D, Grotta JC, Albers GW, Kaste M, Marler JR, Hamilton SA, Tilley BC, Davis SM, Donnan GA, Hacke W, Ecass AN, Group Er‐PS, Allen K, Mau J, Meier D, del Zoppo G, De Silva DA, Butcher KS, Parsons MW, Barber PA, Levi C, Bladin C, Byrnes G. Time to treatment with intravenous alteplase and outcome in stroke: an updated pooled analysis of ECASS, ATLANTIS, NINDS, and EPITHET trials. Lancet. 2010; 375:1695–1703. - PubMed
-
- Ebinger M, Winter B, Wendt M, Weber JE, Waldschmidt C, Rozanski M, Kunz A, Koch P, Kellner PA, Gierhake D, Villringer K, Fiebach JB, Grittner U, Hartmann A, Mackert BM, Endres M, Audebert HJ; STEMO Consortium . Effect of the use of ambulance‐based thrombolysis on time to thrombolysis in acute ischemic stroke: a randomized clinical trial. JAMA. 2014; 311:1622–1631. - PubMed
-
- Kunz A, Ebinger M, Geisler F, Rozanski M, Waldschmidt C, Weber JE, Wendt M, Winter B, Zieschang K, Fiebach JB, Villringer K, Erdur H, Scheitz JF, Tutuncu S, Bollweg K, Grittner U, Kaczmarek S, Endres M, Nolte CH, Audebert HJ. Functional outcomes of pre‐hospital thrombolysis in a mobile stroke treatment unit compared with conventional care: an observational registry study. Lancet Neurol. 2016;15:1035–1043. - PubMed
-
- Weber JE, Ebinger M, Rozanski M, Waldschmidt C, Wendt M, Winter B, Kellner P, Baumann A, Fiebach JB, Villringer K, Kaczmarek S, Endres M, Audebert HJ; STEMO Consortium . Prehospital thrombolysis in acute stroke: results of the PHANTOM‐S pilot study. Neurology. 2013;80:163–168. - PubMed
-
- Itrat A, Taqui A, Cerejo R, Briggs F, Cho SM, Organek N, Reimer AP, Winners S, Rasmussen P, Hussain MS, Uchino K; Cleveland Pre‐Hospital Acute Stroke Treatment Group . Telemedicine in prehospital stroke evaluation and thrombolysis: taking stroke treatment to the doorstep. JAMA Neurol. 2016;73:162–168. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
