

Practice Variation in Anticoagulation Prescription and Outcomes After Device-Detected Atrial Fibrillation
- PMID: 30880434
- PMCID: PMC6652191
- DOI: 10.1161/CIRCULATIONAHA.118.038988
Practice Variation in Anticoagulation Prescription and Outcomes After Device-Detected Atrial Fibrillation
Abstract
Background: Device-detected atrial fibrillation (AF) is associated with increased risk of stroke; however, there are no clearly defined thresholds of AF burden at which to initiate oral anticoagulation (OAC). We sought to describe OAC prescription practice variation in response to new device-detected AF and the association with outcomes.
Methods: We performed a retrospective cohort study using data from the Veterans Health Administration linked to remote monitoring data that included day-level AF burden. We included patients with cardiac implantable electronic devices and remote monitoring from 2011 to 2014, CHA2DS2-VASc score ≥2, and no prior stroke or OAC receipt in the preceding 2 years. We determined the proportion of patients prescribed OAC within 90 days after new device-detected AF across a range of AF thresholds (≥6 minutes to >24 hours) and examined site variation in OAC prescription. We used multivariable Cox proportional hazards regressions to determine the association of OAC prescription with stroke by device-detected AF burden.
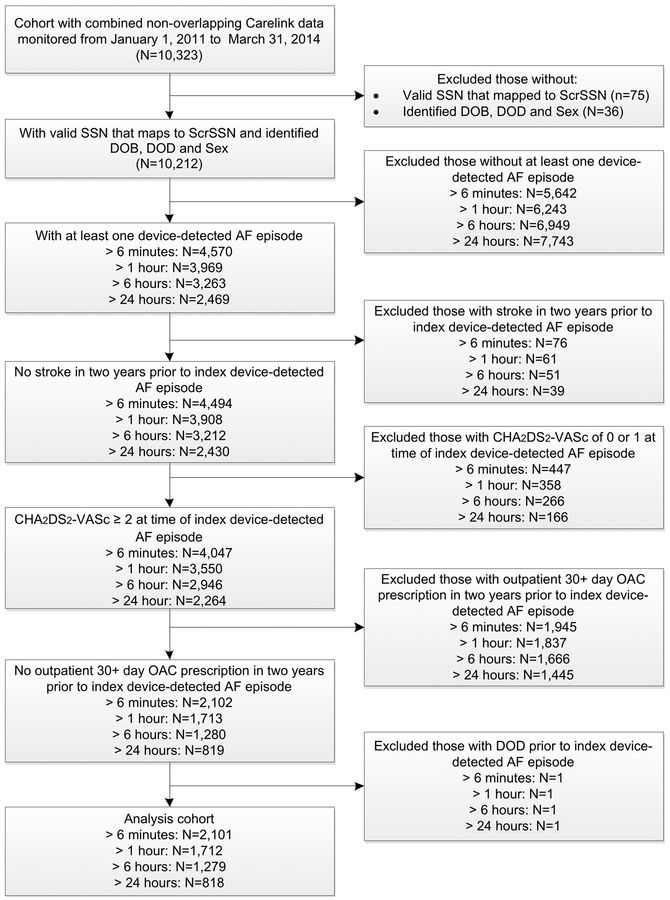
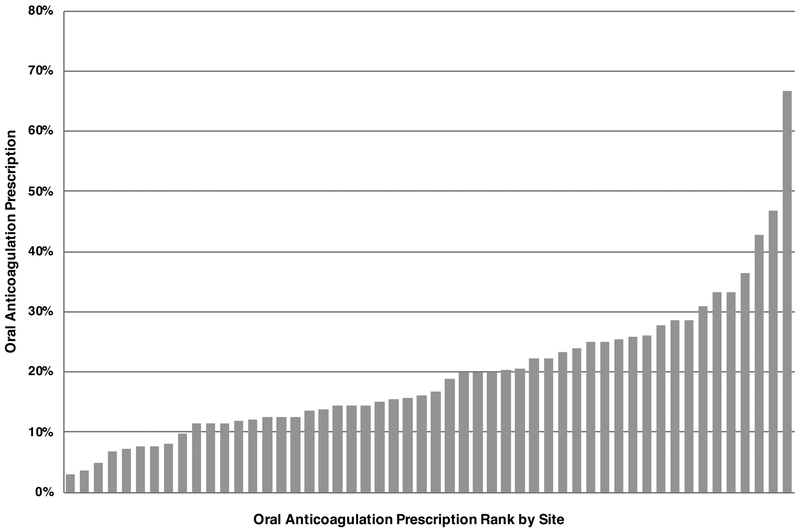
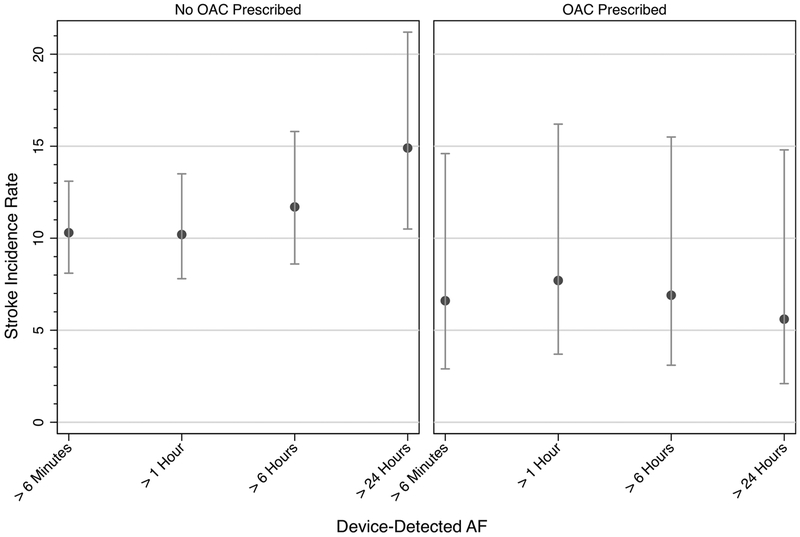
Results: Among 10 212 patients with cardiac implantable electronic devices, 4570 (45%), 3969 (39%), 3263 (32%), and 2469 (24%) had device-detected AF >6 minutes, >1 hour, >6 hours, and >24 hours, respectively. For device-detected AF >1 hour, 1712 patients met inclusion criteria (72±10 years; 1.5% female; CHA2DS2-VASc score 4.0±1.4; HAS-BLED score 2.6±1.1). The proportion receiving OAC varied based on device-detected AF burden (≥6 minutes: 272/2101 [13%]; >1 hour: 273/1712 [16%]; >6 hours: 263/1279 [21%]; >24 hours: 224/818 [27%]). Across 52 sites (N=1329 patients), there was substantial site-level variation in OAC prescription after device-detected AF >1 hour (median, 16%; range, 3%-67%; median odds ratio, 1.56 [95% credible interval, 1.49-1.71]). In adjusted models, OAC prescription after device-detected AF >24 hours was associated with reduced stroke risk (hazard ratio, 0.28; 95% CI, 0.10-0.81; P=0.02), although the propensity-adjusted model was significant when AF lasted at least 6 minutes.
Conclusions: Among veterans with cardiac implantable electronic devices, device-detected AF is common. There is large practice variation in 90-day OAC initiation after new device-detected AF, with low rates of treatment overall, even for episodes that last >24 hours. The strongest association of OAC with reduction in stroke was observed after device-detected AF >24 hours. Randomized trials are needed to confirm these observational findings.
Keywords: atrial fibrillation; stroke.
Figures
Comment in
-
Device-Detected Atrial Fibrillation.Circulation. 2019 May 28;139(22):2513-2515. doi: 10.1161/CIRCULATIONAHA.119.040549. Epub 2019 Mar 17. Circulation. 2019. PMID: 30880437 No abstract available.
References
-
- Connolly SJ, Ezekowitz MD, Yusuf S, Eikelboom J, Oldgren J, Parekh A, Pogue J, Reilly PA, Themeles E, Varrone J, Wang S, Alings M, Xavier D, Zhu J, Diaz R, Lewis BS, Darius H, Diener HC, Joyner CD, Wallentin L, Committee R-LS and Investigators. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361:1139–1151. - PubMed
-
- Go AS, Hylek EM, Chang Y, Phillips KA, Henault LE, Capra AM, Jensvold NG, Selby JV, Singer DE. Anticoagulation therapy for stroke prevention in atrial fibrillation: how well do randomized trials translate into clinical practice? JAMA. 2003;290:2685–2692. - PubMed
-
- January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC, Conti JB, Ellinor PT, Ezekowitz MD, Field ME, Murray KT, Sacco RL, Stevenson WG, Tchou PJ, Tracy CM, Yancy CW, ACC/AHA Task Force Members. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation. 2014;130:e199–267. - PMC - PubMed
-
- Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, Castella M, Diener HC, Heidbuchel H, Hendriks J, Hindricks G, Manolis AS, Oldgren J, Popescu BA, Schotten U, Van Putte B, Vardas P, Agewall S, Camm J, Baron Esquivias G, Budts W, Carerj S, Casselman F, Coca A, De Caterina R, Deftereos S, Dobrev D, Ferro JM, Filippatos G, Fitzsimons D, Gorenek B, Guenoun M, Hohnloser SH, Kolh P, Lip GY, Manolis A, McMurray J, Ponikowski P, Rosenhek R, Ruschitzka F, Savelieva I, Sharma S, Suwalski P, Tamargo JL, Taylor CJ, Van Gelder IC, Voors AA, Windecker S, Zamorano JL, Zeppenfeld K. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J. 2016;37:2893–2962. - PubMed
-
- Vanassche T, Lauw MN, Eikelboom JW, Healey JS, Hart RG, Alings M, Avezum A, Diaz R, Hohnloser SH, Lewis BS, Shestakovska O, Wang J, Connolly SJ. Risk of ischaemic stroke according to pattern of atrial fibrillation: analysis of 6563 aspirin-treated patients in ACTIVE-A and AVERROES. Eur Heart J. 2015;36:281–287a. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
