

Right ventricular outflow tract velocity time integral-to-pulmonary artery systolic pressure ratio: a non-invasive metric of pulmonary arterial compliance differs across the spectrum of pulmonary hypertension
- PMID: 30880577
- PMCID: PMC6540515
- DOI: 10.1177/2045894019841978
Right ventricular outflow tract velocity time integral-to-pulmonary artery systolic pressure ratio: a non-invasive metric of pulmonary arterial compliance differs across the spectrum of pulmonary hypertension
Abstract
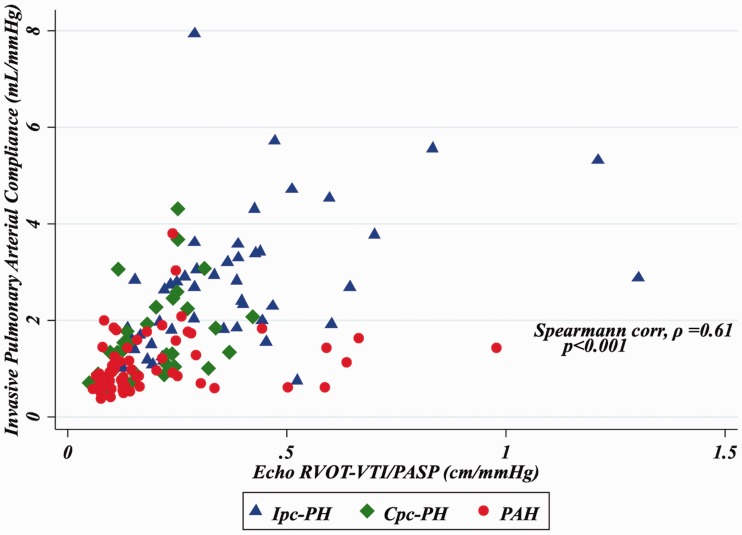
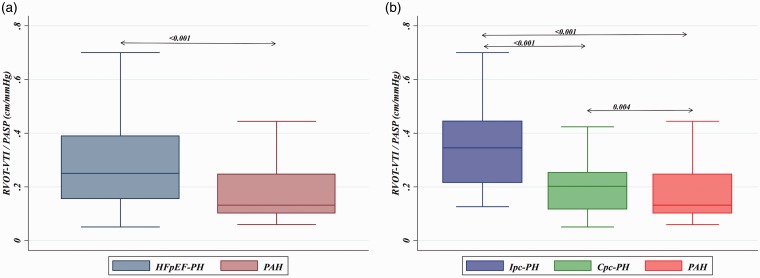
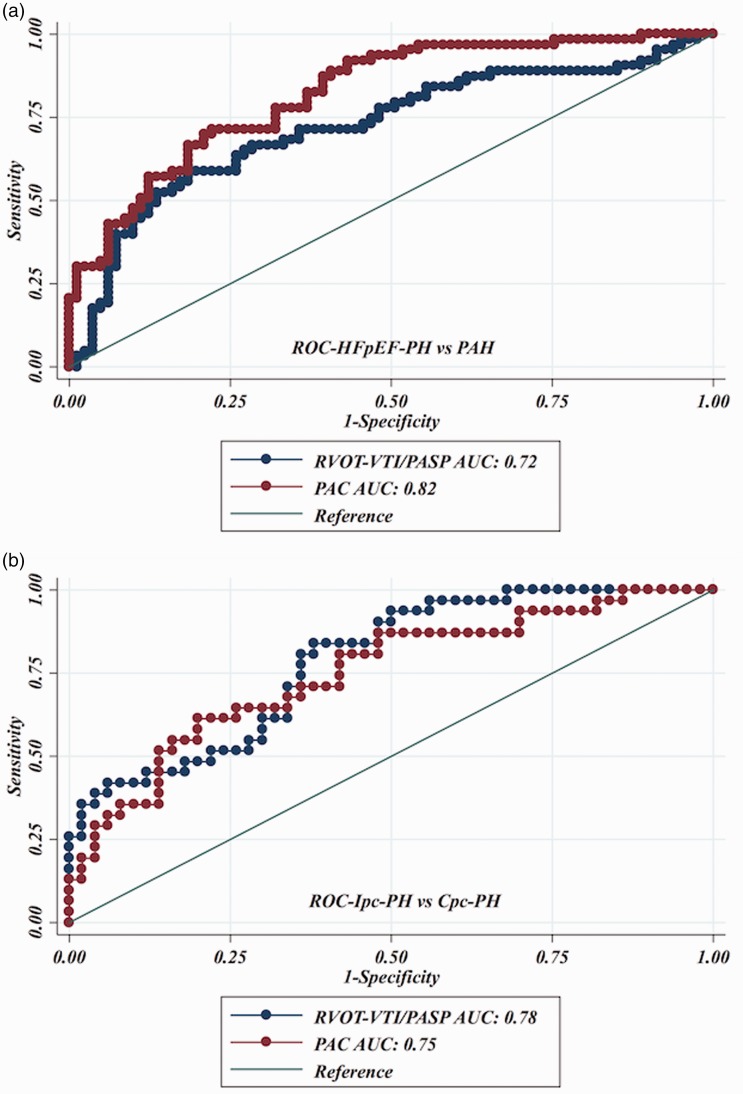
Pulmonary arterial compliance (PAC), invasively assessed by the ratio of stroke volume to pulmonary arterial (PA) pulse pressure, is a sensitive marker of right ventricular (RV)-PA coupling that differs across the spectrum of pulmonary hypertension (PH) and is predictive of outcomes. We assessed whether the echocardiographically derived ratio of RV outflow tract velocity time integral to PA systolic pressure (RVOT-VTI/PASP) (a) correlates with invasive PAC, (b) discriminates heart failure with preserved ejection-associated PH (HFpEF-PH) from pulmonary arterial hypertension (PAH), and (c) is associated with functional capacity. We performed a retrospective cohort study of patients with PAH (n = 70) and HFpEF-PH (n = 86), which was further dichotomized by diastolic pressure gradient (DPG) into isolated post-capillary PH (DPG < 7 mmHg; Ipc-PH, n = 54), and combined post- and pre-capillary PH (DPG ≥ 7 mm Hg; Cpc-PH, n = 32). Of the 156 patients, 146 had measurable RVOT-VTI or PASP and were included in further analysis. RVOT-VTI/PASP correlated with invasive PAC overall (ρ = 0.61, P < 0.001) and for the PAH (ρ = 0.38, P = 0.002) and HFpEF-PH (ρ = 0.63, P < 0.001) groups individually. RVOT-VTI/PASP differed significantly across the PH spectrum (PAH: 0.13 [0.010-0.25] vs. Cpc-PH: 0.20 [0.12-0.25] vs. Ipc-PH: 0.35 [0.22-0.44]; P < 0.001), distinguished HFpEF-PH from PAH (AUC = 0.72, 95% CI = 0.63-0.81) and Cpc-PH from Ipc-PH (AUC = 0.78, 95% CI = 0.68-0.88), and remained independently predictive of 6-min walk distance after multivariate analysis (standardized β-coefficient = 27.7, 95% CI = 9.2-46.3; P = 0.004). Echocardiographic RVOT-VTI/PASP is a novel non-invasive metric of PAC that differs across the spectrum of PH. It distinguishes the degree of pre-capillary disease within HFpEF-PH and is predictive of functional capacity.
Keywords: Cpc-PH; non-invasive; pulmonary arterial compliance; pulmonary hypertension.
Figures
References
-
- Galie N, Humbert M, Vachiery JL, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Heart J 2016; 37: 67–119. - PubMed
-
- Vachiery JL, Adir Y, Barbera JA, et al. Pulmonary hypertension due to left heart diseases. J Am Coll Cardiol 2013; 62: D100–108. - PubMed
-
- Gerges M, Gerges C, Pistritto AM, et al. Pulmonary hypertension in heart failure. Epidemiology, right ventricular function, and survival. Am J Respir Crit Care Med 2015; 192: 1234–1246. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
