

Bilateral versus unilateral cryptorchidism in nonobstructive azoospermia: Testicular sperm extraction outcomes
- PMID: 30880688
- PMCID: PMC6732891
- DOI: 10.4103/aja.aja_2_19
Bilateral versus unilateral cryptorchidism in nonobstructive azoospermia: Testicular sperm extraction outcomes
Abstract
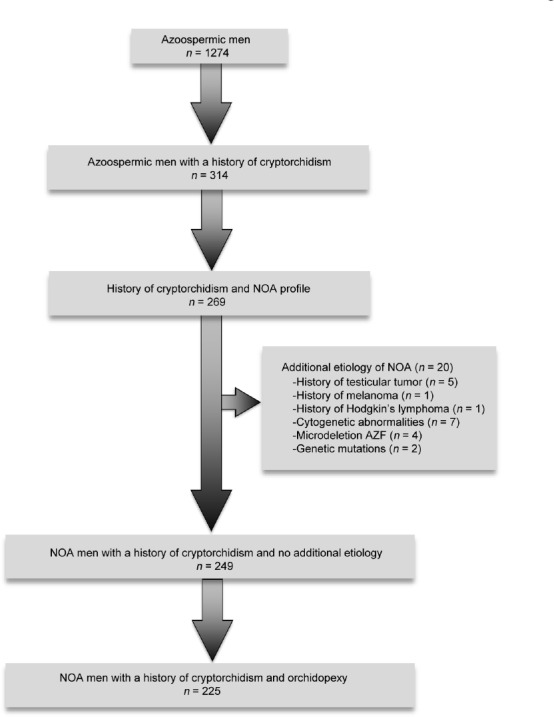
Cryptorchidism is one of the most frequent causes of nonobstructive azoospermia (NOA) in adulthood. Although it is well known that spermatogenesis is more impaired in bilateral than in unilateral cryptorchidism, previous studies have only described small cohorts or inhomogeneous population. Consequently, we analyzed a cohort of 225 men with only a history of cryptorchidism as sole etiopathogenetic factor for NOA, and compared testicular sperm extraction (TESE) outcomes between men with bilateral versus unilateral cryptorchidism. Our results show no difference in follicle-stimulating hormone (FSH) levels and testicular volumes between men with a history of bilateral cryptorchidism compared to unilateral cryptorchidism (median: 21.3 IU l-1 vs 19.3 IU l-1, P = 0.306; and 7.2 ml vs 7.9 ml, P = 0.543, respectively). In addition, sperm retrieval rates were similar (66.2% vs 60.0%, P = 0.353). Using multivariate analysis, we have found that only a low inhibin B level (above the assay's detection limit) was positively associated with successful sperm retrieval (P < 0.05). Regarding intracytoplasmic sperm injection outcomes, we found that cumulative pregnancy rate and live birth rate per cycle were not statistically different between the two groups (17.4% vs 27.8%, P = 0.070; and 16.1% vs 26.4%, P = 0.067, respectively). Unexpectedly, there was no significant difference in hormonal profiles (FSH, luteinizing hormone [LH], testosterone, and inhibin B levels) and TESE outcomes between unilateral versus bilateral cryptorchidism. This suggests that a history of unilateral cryptorchidism could reflect a bilateral testicular impairment. Interestingly, inhibin B level might be a predictor of successful TESE.
Keywords: cryptorchidism; intracytoplasmic sperm injection; nonobstructive azoospermia; testicular sperm extraction.
Conflict of interest statement
None
Figures
References
-
- Barthold JS, González R. The epidemiology of congenital cryptorchidism, testicular ascent and orchiopexy. J Urol. 2003;170:2396–401. - PubMed
-
- Averous M, Lopez C. Cryptorchidism: the point of view of a pediatric urologist. Gynecol Obstet Fertil. 2004;32:813–7. [Article in French] - PubMed
-
- Hadziselimovic F. Opinion: comment on evaluation and treatment of cryptorchidism: AUA/AAP and Nordic consensus guidelines. Urol Int. 2016;96:249–54. - PubMed
-
- Olesen IA, Andersson AM, Aksglaede L, Skakkebaek NE, Rajpert-de Meyts E, et al. Clinical, genetic, biochemical, and testicular biopsy findings among 1,213 men evaluated for infertility. Fertil Steril. 2017;107:74–82.e7. - PubMed
-
- Fedder J, Cruger D, Oestergaard B, Petersen GB. Etiology of azoospermia in 100 consecutive nonvasectomized men. Fertil Steril. 2004;82:1463–5. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
