

Prevalence and factors associated with suboptimal peak inspiratory flow rates in COPD
- PMID: 30880948
- PMCID: PMC6402615
- DOI: 10.2147/COPD.S195438
Prevalence and factors associated with suboptimal peak inspiratory flow rates in COPD
Abstract
Purpose: Adequate peak inspiratory flow rate (PIFR) is required for drug dispersion with dry powder inhalers (DPIs). Prevalence of PIFR discordance (suboptimal PIFR with prescribed inhalers) and factors influencing device-specific PIFR are unclear in COPD. The objective of this study was to determine the prevalence of PIFR discordance and associated clinical factors in a stable COPD population.
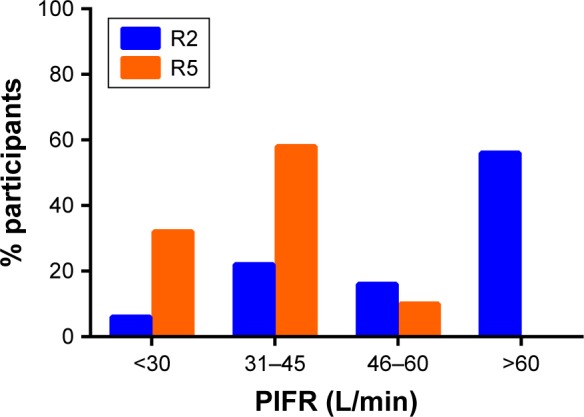
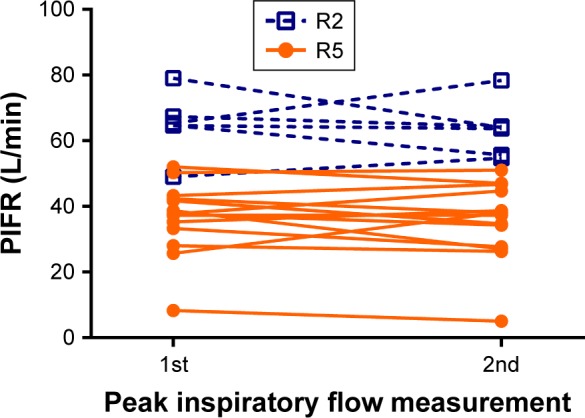
Patients and methods: An observational, single-center, cohort study was conducted including 66 outpatients with COPD. PIFR was measured using the In-Check™ Dial with applied resistance of prescribed inhalers. Participants were defined as discordant if measured PIFR was <30 L/min and <60 L/min for high and low-medium resistance devices, respectively, using an inspiratory effort the participant normally used with their prescribed DPI.
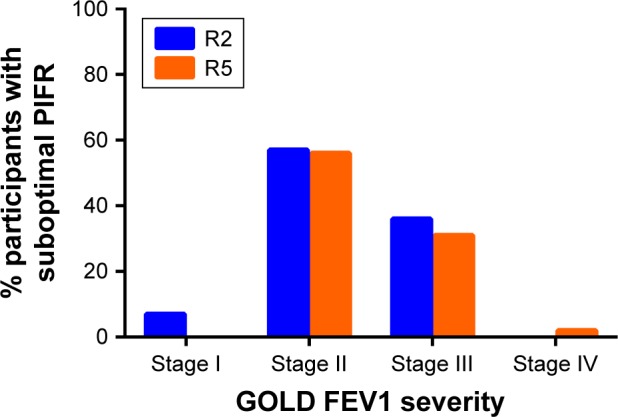
Results: The median age of the COPD participants was 69.4 years, 92% were white and 47% were female. A total of 48% were using low-medium resistance DPIs (Diskus®/Ellipta®) and 76% used high-resistance DPI (Handihaler®). A total of 40% of COPD participants were discordant to prescribed inhalers. Female gender was the only factor consistently associated with lower PIFR. Shorter height was associated with reduced PIFR for low-medium resistance (r=0.44; P=0.01), but not high resistance (r=0.20; P=0.16). There was no correlation between PIFR by In-Check™ dial and PIFR measured by standard spirometer.
Conclusion: PIFR is reduced in stable COPD patients, with female gender being the only factor consistently associated with reduced PIFR. Discordance with prescribed inhalers was seen in 40% of COPD patients, suggesting that many COPD patients do not generate adequate inspiratory force to overcome prescribed DPIs resistance in the course of normal use.
Keywords: chronic obstructive; drug delivery systems; dry powder inhaler; peak inspiratory flow rate; pulmonary disease.
Conflict of interest statement
Disclosure RAP has research support from Boehringer-Ingelheim and GlaxoSmithKline, served on Advisory Board for GlaxoSmithKline and Teva, has served as speaker for AstraZeneca and Sunovion, and served on Data Safety Monitoring Board for Grifols. JAO has performed advisory consulting for Boehringer-Ingelheim, GlaxoSmithKline, Theravance, Novartis, and AstraZeneca. She also has an investigator-initiated research grant from Sunovion. JFD has served as advisor to AZ, GSK, Novartis, Mylan, Sunovion, and Theravance. MBD has performed advisory consulting for Boehringer-Ingelheim, GlaxoSmithKline, and AstraZeneca. There were no funders, thus no funders had a role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; and in the decision to publish the results. SG reports no conflicts of interest in this work.
Figures
References
-
- Global strategy for prevention, diagnosis, and management of COPD. 2018. [Accessed November 5, 2018]. Available from: www.goldcopd.org.
-
- FDA approved drugs for pulmonary/respiratory diseases. [Accessed November 5, 2018]. Available from: https://www.centerwatch.com/drug-information/fda-approved-drugs/therapeu....
-
- Pitcairn G, Reader S, Pavia D, Newman S. Deposition of corticosteroid aerosol in the human lung by Respimat soft mist inhaler compared to deposition by metered dose inhaler or by Turbuhaler dry powder inhaler. J Aerosol Med. 2005;18(3):264–272. - PubMed
-
- Clark AR, Hollingworth AM. The relationship between powder inhaler resistance and peak inspiratory conditions in healthy volunteers – implications for in vitro testing. J Aerosol Med. 1993;6(2):99–110. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
