

Iatrogenic bile duct injury: impact and management challenges
- PMID: 30881079
- PMCID: PMC6408920
- DOI: 10.2147/CEG.S169492
Iatrogenic bile duct injury: impact and management challenges
Abstract
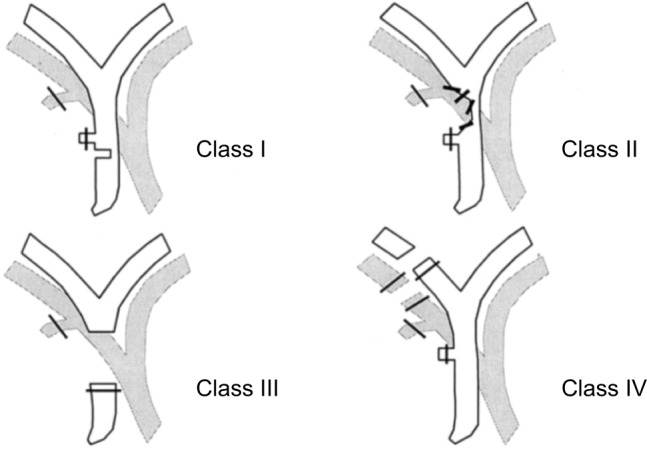
Iatrogenic bile duct injuries (BDIs) after laparoscopic cholecystectomy, being one of the most common performed surgical procedures, remain a substantial problem in gastrointestinal surgery with a significant impact on patient's quality of life. The primary aim of this review was to discuss the classification of BDIs, the proposed methods to prevent biliary lesions, the associated risk factors, and the management challenges depending on the timing of recognition of the injury, its extension, the patient's clinical condition, and the availability of experienced hepatobiliary surgeons. Early recognition of BDI is of paramount importance and limiting the diagnosis delay is crucial for an optimal postoperative outcome. The therapeutic management depends on the type and gravity of the biliary lesion, and includes endoscopic, radiologic, and surgical approaches.
Keywords: bile duct injury; biliary anatomy; early recognition; endoscopic treatment; laparoscopic cholecystectomy; management challenge; surgical repair.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures
References
-
- Pesce A, Portale TR, Minutolo V, Scilletta R, Li Destri G, Puleo S. Bile duct injury during laparoscopic cholecystectomy without intraoperative cholangiography: a retrospective study on 1,100 selected patients. Dig Surg. 2012;29(4):310–314. - PubMed
-
- Woods MS. Estimated costs of biliary tract complications in laparoscopic cholecystectomy based upon Medicare cost/charge ratios. A case-control study. Surg Endosc. 1996;10(10):1004–1007. - PubMed
-
- Carroll BJ, Birth M, Phillips EH. Common bile duct injuries during laparoscopic cholecystectomy that result in litigation. Surg Endosc. 1998;12(4):310–314. - PubMed
-
- Bismuth H, Majno PE. Biliary strictures: classification based on the principles of surgical treatment. World J Surg. 2001;25(10):1241–1244. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
