

Breakdown of Autonomously Functioning Thyroid Nodule Accompanied by Acromegaly After Octreotide Treatment
- PMID: 30881346
- PMCID: PMC6405443
- DOI: 10.3389/fendo.2019.00131
Breakdown of Autonomously Functioning Thyroid Nodule Accompanied by Acromegaly After Octreotide Treatment
Abstract
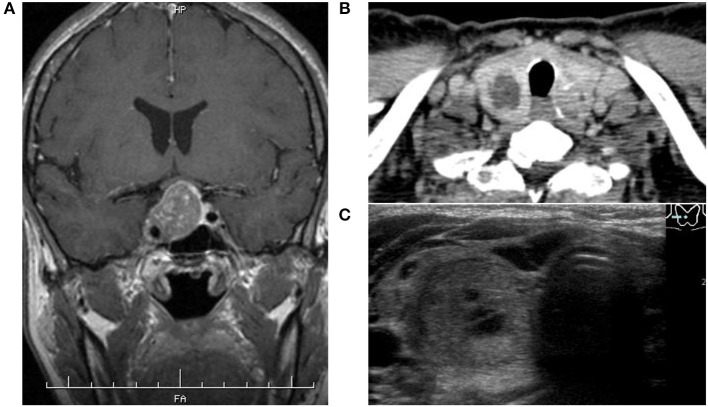
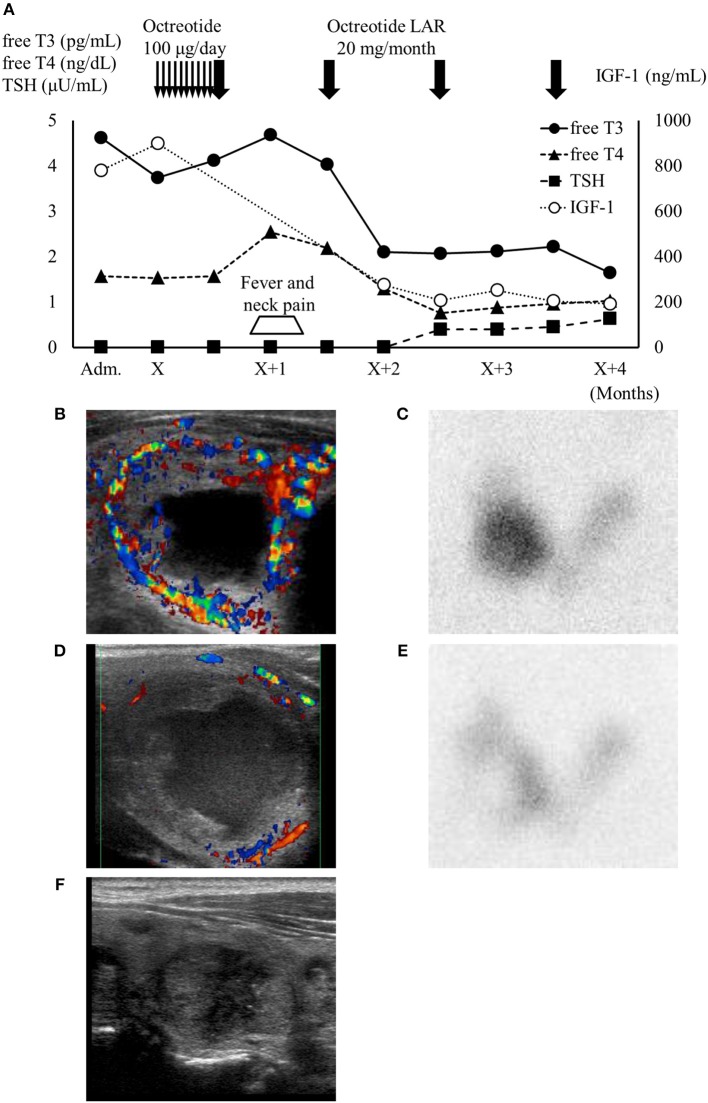
Patients with acromegaly are at increased risk of developing certain tumors, including goiter and thyroid nodules, and occasionally autonomous thyroid nodules. A 53-year-old woman presented at our hospital with untreated acromegaly. She had typical physical features of acromegaly with pituitary adenoma, and thyrotoxicosis with thyroid-stimulating hormone suppression was also confirmed. Thyroid ultrasonography and scintigraphy showed an autonomously functioning thyroid nodule on her right lobe. Because her thyrotoxicosis was mild, she was initially treated with octreotide for acromegaly. However, 1 month after octreotide administration, she developed neck pain and fever with transient thyrotoxicosis. The blood flow around the nodule then decreased and the excess trapping of isotope detected by scintigraphy was reduced, followed by normalization of insulin-like growth factor-1 levels and thyroid function. This case suggests that octreotide may have unexpected effects on autonomous thyroid nodules. However, further studies are needed to determine the clinical course of autonomously functioning thyroid nodules, including thyroid function and tumor manifestations, during octreotide therapy.
Keywords: acromegaly; autonomously functioning thyroid nodule; pituitary adenoma; somatostatin analog; thyrotoxicosis.
Figures
Similar articles
-
Challenges in the functional diagnosis of thyroid nodules before surgery for TSH-producing pituitary adenoma.Endocrinol Diabetes Metab Case Rep. 2021 Apr 1;2021:20-0221. doi: 10.1530/EDM-20-0221. Online ahead of print. Endocrinol Diabetes Metab Case Rep. 2021. PMID: 33929339 Free PMC article.
-
Real-time elastography in autonomously functioning thyroid nodules: relationship with TSH levels, scintigraphy, and ultrasound patterns.Endocrine. 2017 Dec;58(3):488-494. doi: 10.1007/s12020-017-1277-6. Epub 2017 Mar 11. Endocrine. 2017. PMID: 28285385
-
A pregnant woman with an autonomously functioning thyroid nodule: a case report.Gynecol Endocrinol. 2020 Dec;36(12):1140-1143. doi: 10.1080/09513590.2020.1822798. Epub 2020 Sep 21. Gynecol Endocrinol. 2020. PMID: 32954874
-
Medical treatment of acromegaly: comorbidities and their reversibility by somatostatin analogs.Neuroendocrinology. 2006;83(3-4):249-57. doi: 10.1159/000095535. Epub 2006 Oct 13. Neuroendocrinology. 2006. PMID: 17047390 Review.
-
Somatostatin analogues in acromegaly and gastroenteropancreatic neuroendocrine tumours: past, present and future.Endocr Relat Cancer. 2016 Dec;23(12):R551-R566. doi: 10.1530/ERC-16-0151. Epub 2016 Oct 3. Endocr Relat Cancer. 2016. PMID: 27697899 Review.
Cited by
-
Growth hormone-secreting pituitary adenoma combined with Graves' disease: retrospective case series and literature review.Endocr Connect. 2024 Mar 4;13(4):e230439. doi: 10.1530/EC-23-0439. Print 2024 Apr 1. Endocr Connect. 2024. PMID: 38349236 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources