

Best Practices for Evaluation and Treatment of Agitated Children and Adolescents (BETA) in the Emergency Department: Consensus Statement of the American Association for Emergency Psychiatry
- PMID: 30881565
- PMCID: PMC6404720
- DOI: 10.5811/westjem.2019.1.41344
Best Practices for Evaluation and Treatment of Agitated Children and Adolescents (BETA) in the Emergency Department: Consensus Statement of the American Association for Emergency Psychiatry
Erratum in
-
Erratum: This Article Corrects: "Best Practices for Evaluation and Treatment of Agitated Children and Adolescents (BETA) in the Emergency Department: Consensus Statement of the American Association for Emergency Psychiatry".West J Emerg Med. 2019 May;20(3):537. doi: 10.5811/westjem.2019.4.43550. Epub 2019 Feb 19. West J Emerg Med. 2019. PMID: 31123557 Free PMC article.
-
Erratum: This Article Corrects: "Best Practices for Evaluation and Treatment of Agitated Children and Adolescents (BETA) in the Emergency Department: Consensus Statement of the American Association for Emergency Psychiatry".West J Emerg Med. 2019 Jul;20(4):688-689. doi: 10.5811/westjem.2019.4.44160. Epub 2019 Jul 2. West J Emerg Med. 2019. PMID: 31316711 Free PMC article.
Abstract
Introduction: Agitation in children and adolescents in the emergency department (ED) can be dangerous and distressing for patients, family and staff. We present consensus guidelines for management of agitation among pediatric patients in the ED, including non-pharmacologic methods and the use of immediate and as-needed medications.
Methods: Using the Delphi method of consensus, a workgroup comprised of 17 experts in emergency child and adolescent psychiatry and psychopharmacology from the the American Association for Emergency Psychiatry and the American Academy of Child and Adolescent Psychiatry Emergency Child Psychiatry Committee sought to create consensus guidelines for the management of acute agitation in children and adolescents in the ED.
Results: Consensus found that there should be a multimodal approach to managing agitation in the ED, and that etiology of agitation should drive choice of treatment. We describe general and specific recommendations for medication use.
Conclusion: These guidelines describing child and adolescent psychiatry expert consensus for the management of agitation in the ED may be of use to pediatricians and emergency physicians who are without immediate access to psychiatry consultation.
Conflict of interest statement
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. No author has professional or financial relationships with any companies that are relevant to this study. There are no conflicts of interest or sources of funding to declare.
Figures
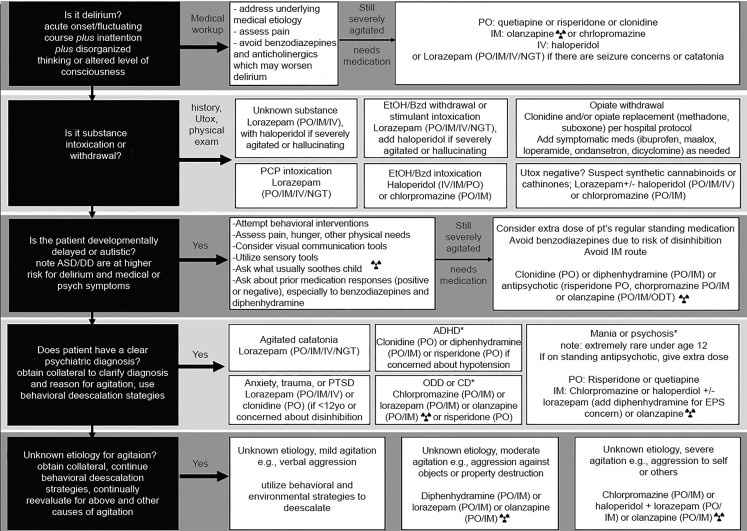
 Do not give olanzapine and benzodiazepines within one hour of each other.
Do not give olanzapine and benzodiazepines within one hour of each other.References
-
- Malas N, Spital L, Fischer J, et al. National Survey on Pediatric Acute Agitation and Behavioral Escalation in Academic Inpatient Pediatric Care Settings. Psychosomatics. 2017;58(3):299–306. - PubMed
-
- Dorfman DH, Kastner B. The use of restraint for pediatric psychiatric patients in emergency departments. Pediatr Emerg Care. 2004;20(3):151–6. - PubMed
-
- Dorfman DH, Mehta SD. Restraint use for psychiatric patients in the pediatric emergency department. Pediatr Emerg Care. 2006;22(1):7–12. - PubMed
-
- Weiss EM. Deadly restraint: a Hartford Courant investigative report. Hartford Courant. 1998
-
- Department of Health and Human Services Centers for Medicare and Medicaid. 42 CRF Part 482 and 483. Medicare and Medicaid Programs; Hospital Conditions of Participation: Patients’ Rights; Final Rule. [Accessed November 22, 2017]. Available at: https://www.cms.gov/Regulations-and-Guidance/Legislation/CFCsAndCoPs/dow....