

Limb Lengthening with a Submuscular Locking Plate
- PMID: 30881755
- PMCID: PMC6407959
- DOI: 10.2106/JBJS.ST.M.00041
Limb Lengthening with a Submuscular Locking Plate
Abstract
Introduction: Limb-lengthening with a submuscular locking plate provides a good alternative for patients, especially children, in whom lengthening over an intramedullary nail would be difficult.
Step 1 external fixation for lengthening with submuscular plating: The first operation is divided into two steps, submuscular plating and external fixation with corticotomy; due to the anatomical characteristics, the procedures differ in the tibia and femur.
Step 2 lengthening: Start distraction at seven to ten days after surgery and continue until the target length is achieved.
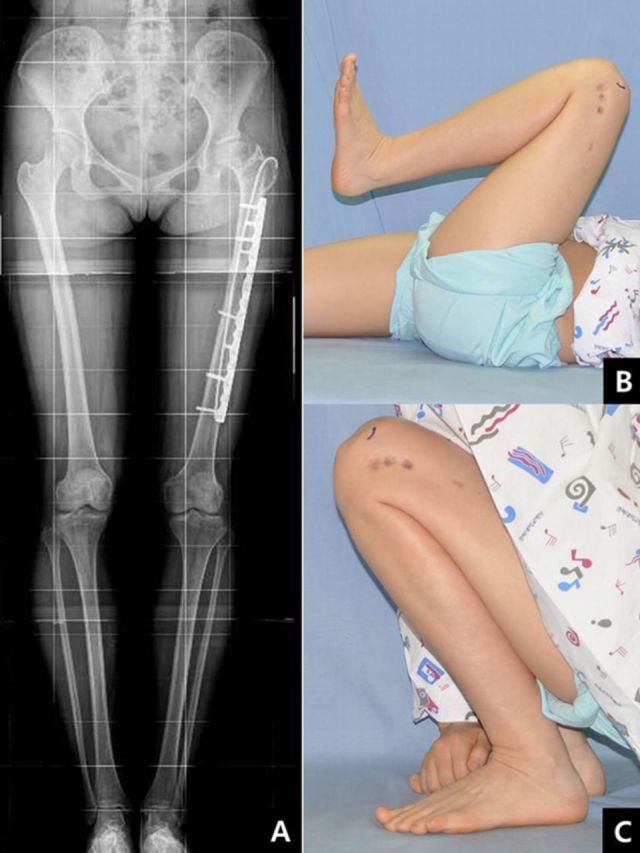
Step 3 locking of the distal segment and removal of the external fixator: When the target length has been achieved, place screws into the distal segment through plate holes and remove the fixator.
Step 4 postoperative care: Start with partial weight-bearing, obtain a radiograph every four to eight weeks, and allow full weight-bearing with crutches when osseous consolidation is observed.
Results: We prospectively performed limb lengthening using an external fixator and a submuscular locking plate in ten patients16.IndicationsContraindicationsPitfalls & Challenges.
Figures












References
-
- Ilizarov GA. The principles of the Ilizarov method. Bull Hosp Jt Dis Orthop Inst. 1988 Spring;48(1):1-11. - PubMed
-
- Price CT Mann JW. Experience with the Orthofix device for limb lengthening. Orthop Clin North Am. 1991 Oct;22(4):651-61. - PubMed
-
- Stanitski DF Shahcheraghi H Nicker DA Armstrong PF. Results of tibial lengthening with the Ilizarov technique. J Pediatr Orthop. 1996 Mar-Apr;16(2):168-72. - PubMed
-
- Zarzycki D Tesiorowski M Zarzycka M Kacki W Jasiewicz B. Long-term results of lower limb lengthening by the Wagner method. J Pediatr Orthop. 2002 May-Jun;22(3):371-4. - PubMed
-
- Paley D. Problems, obstacles, and complications of limb lengthening by the Ilizarov technique. Clin Orthop Relat Res. 1990 Jan;(250):81-104. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials