

Effect of Documenting Prognosis on the Information Provided to ICU Proxies: A Randomized Trial
- PMID: 30882479
- PMCID: PMC6897298
- DOI: 10.1097/CCM.0000000000003731
Effect of Documenting Prognosis on the Information Provided to ICU Proxies: A Randomized Trial
Abstract
Objectives: The Critical Care Choosing Wisely Task Force recommends that intensivists offer patients at high risk for death or severe functional impairment the option of pursuing care focused on comfort. We tested the a priori hypothesis that intensivists who are prompted to document patient prognosis are more likely to disclose prognosis and offer comfort-focused care.
Design: Randomized controlled trial (clinicaltrials.gov: NCT02721810).
Setting: High-fidelity Simulation Center in Baltimore, MD.
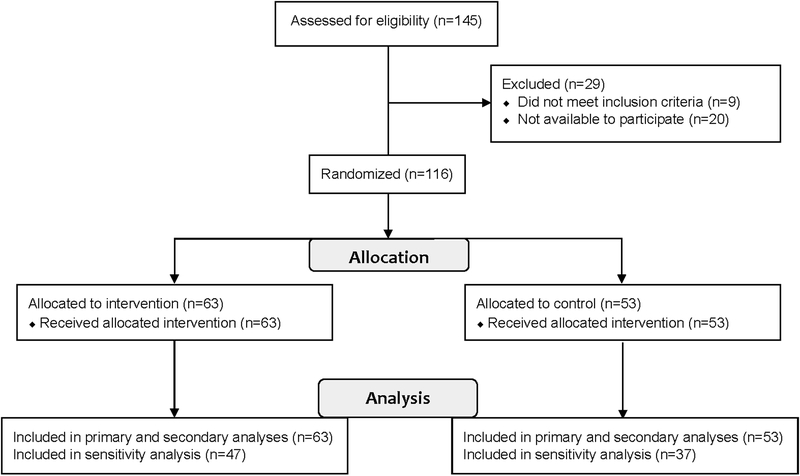
Participants: One hundred sixteen intensivists from 17 states.
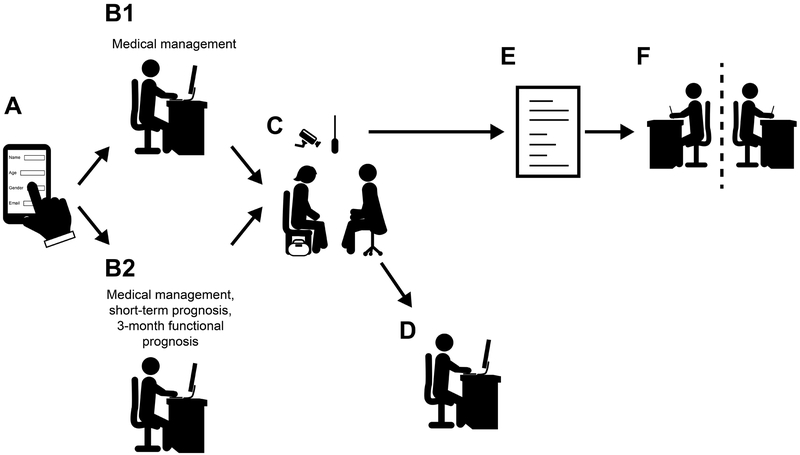
Intervention: All intensivists reviewed a paper-based medical record for a hypothetical patient on ICU day 3 and answered four survey questions about the patient's medical management. Intensivists randomized to the intervention group answered three additional questions about patient prognosis. Thereafter, each intensivist participated in a standardized, video-recorded, simulated family meeting with an actor performing a standardized portrayal of the patient's daughter.
Measurements and main results: Two blinded intensivists reviewed deidentified written transcripts of all simulated family meetings. The primary outcome was the blinded reviewers' assessment that the intensivist had presented the option of care focused entirely on comfort. Secondary outcomes included disclosing risk of death. All outcomes were planned prior to data collection. Among the 63 intensivists randomized to the intervention, 50 (79%) expected the patient to die during the hospitalization and 58 (92%) expected the patient to have new functional impairments preventing independent living. Intensivists in the intervention versus control group were no more likely to offer the option of care focused on comfort (13% vs 13%; 95% CI, -13% to 12%; p = 1.0) but were more likely to inform the daughter that her father was sick enough to die (68% vs 43%; 95% CI, 5-44%; p = 0.01).
Conclusions: Documenting prognosis may help intensivists disclose prognosis to ICU proxies, but in isolation, it is unlikely to change the treatment options offered during initial family meetings.
Figures
Comment in
-
SCIP-ping Over Opportunities to Discuss Comfort Care With ICU Families.Crit Care Med. 2019 Jun;47(6):865-867. doi: 10.1097/CCM.0000000000003756. Crit Care Med. 2019. PMID: 31095015 No abstract available.
-
End-of-Life Care in the ICU.Am J Respir Crit Care Med. 2021 Mar 15;203(6):756-758. doi: 10.1164/rccm.202008-3071RR. Am J Respir Crit Care Med. 2021. PMID: 33497587 No abstract available.
References
-
- Fried TR, Bradley EH, Towle VR, et al.: Understanding the treatment preferences of seriously ill patients. N Engl J Med 2002; 346: 1061–1066 - PubMed
-
- Somogyi-Zalud E, Zhong Z, Hamel MB, et al.: The use of life-sustaining treatments in hospitalized persons aged 80 and older. J Am Geriatr Soc 2002; 50:930–934 - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
