

Comparison of 1-year clinical outcomes between prasugrel and ticagrelor versus clopidogrel in type 2 diabetes patients with acute myocardial infarction underwent successful percutaneous coronary intervention
- PMID: 30882670
- PMCID: PMC6426627
- DOI: 10.1097/MD.0000000000014833
Comparison of 1-year clinical outcomes between prasugrel and ticagrelor versus clopidogrel in type 2 diabetes patients with acute myocardial infarction underwent successful percutaneous coronary intervention
Abstract
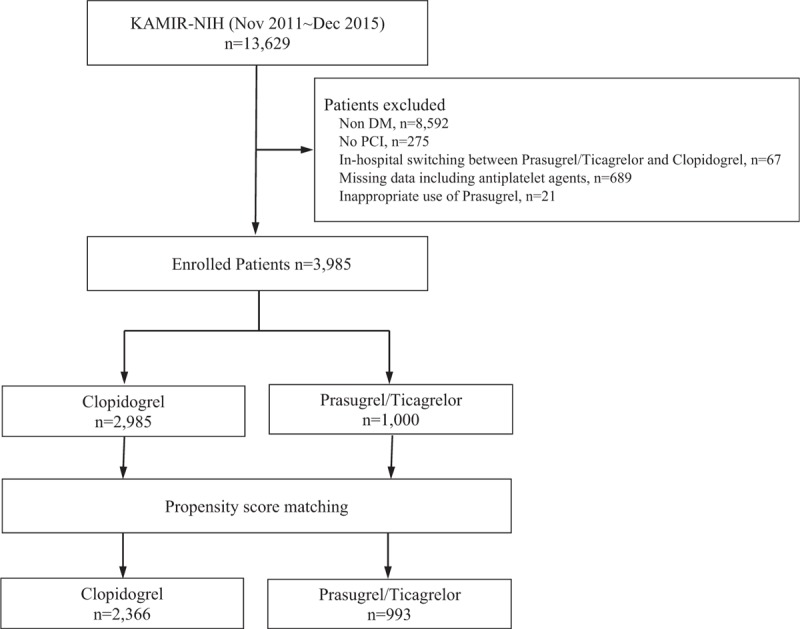
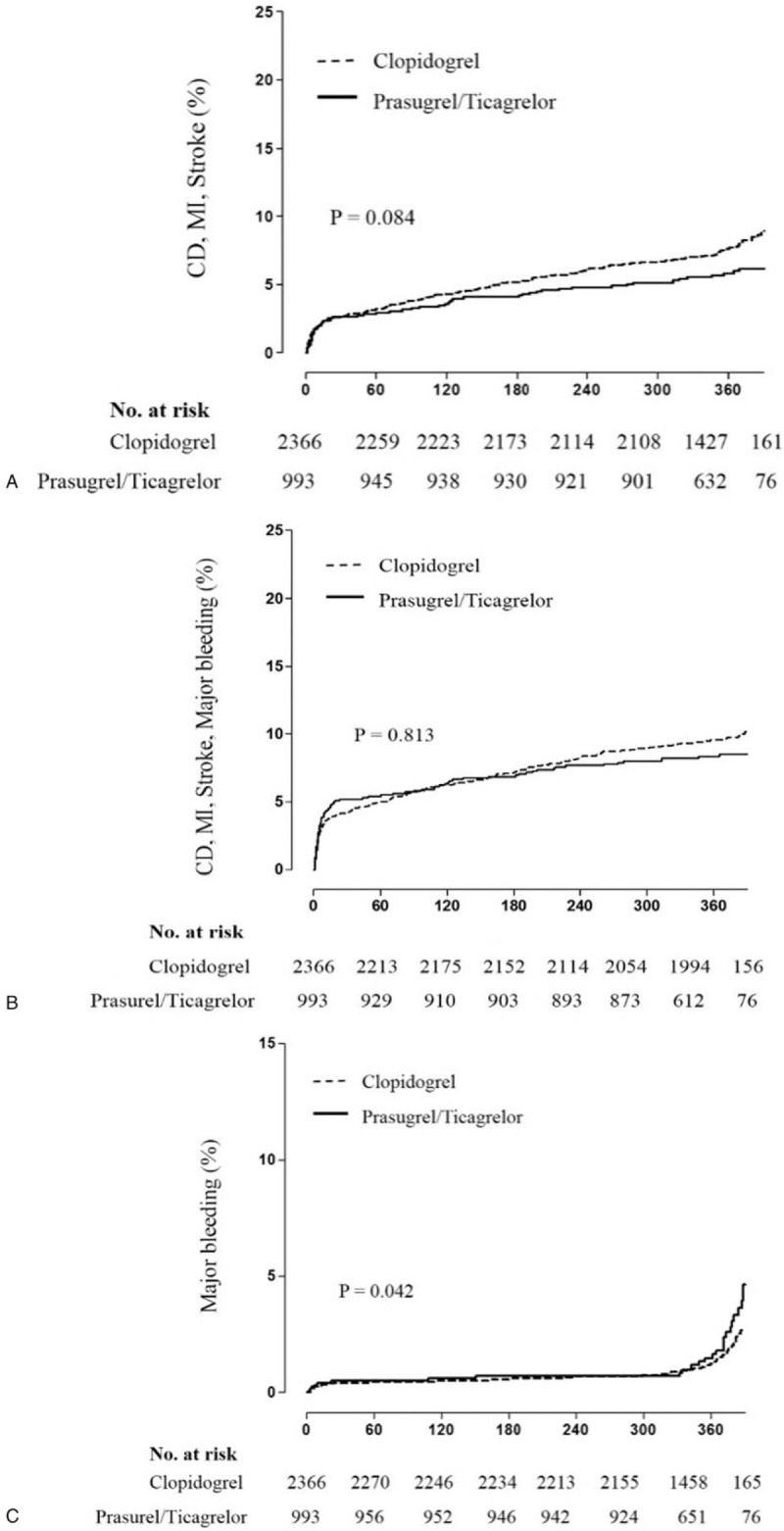
Although the new oral P2Y12 inhibitors, prasugrel/ticagrelor have shown greater efficacy than clopidogrel in patients with the acute coronary syndrome, but they have not shown better efficacy in Korean patients. So we evaluated the efficacy of the prasugrel/ticagrelor in patients with myocardial infarction (MI) and diabetes, a more high-risk patients group.From the Korea Acute Myocardial Infarction Registry-National Institute of Health, 3985 patients with MI and diabetes who underwent PCI were enrolled between November 2011 and December 2015. The patients were divided into 2 groups: clopidogrel (n = 2985) and prasugrel/ticagrelor (n = 1000).After propensity score matching, prasugrel/ticagrelor group showed a no significant difference in risk of the composite of cardiac death (CD), recurrent MI or stroke (hazard ratio [HR], 0.705; 95% confidence interval [CI], 0.474-1.048; P = .084). However, the risk of major bleeding was significantly higher in the prasugrel/ticagrelor group. (HR; 2.114, 95% CI; [1.027-4.353], P = .042). In subgroup analysis, major bleeding was significantly increased in the subgroup of creatinine clearance <60 ml/min/1.73 m, hypertension, underwent a trans-femoral approach and diagnosed as NSTEMI among the prasugrel/ticagrelor group.The use of prasugrel/ticagrelor did not improve the composite of CD, recurrent MI or stroke, however, significantly increased major bleeding events in Korean patients with MI and diabetes undergoing PCI.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures
Similar articles
-
Efficacy and Safety of Clopidogrel, Prasugrel and Ticagrelor in ACS Patients Treated with PCI: A Propensity Score Analysis of the RENAMI and BleeMACS Registries.Am J Cardiovasc Drugs. 2020 Jun;20(3):259-269. doi: 10.1007/s40256-019-00373-1. Am J Cardiovasc Drugs. 2020. PMID: 31586336
-
Prasugrel versus ticagrelor in patients with myocardial infarction undergoing percutaneous coronary intervention.Heart. 2021 Jul;107(14):1145-1151. doi: 10.1136/heartjnl-2020-318694. Epub 2021 Mar 12. Heart. 2021. PMID: 33712510 Free PMC article.
-
Comparative effectiveness and safety of antiplatelet drugs in patients with diabetes mellitus and acute coronary syndrome.Pharmacoepidemiol Drug Saf. 2018 Dec;27(12):1361-1370. doi: 10.1002/pds.4668. Epub 2018 Oct 31. Pharmacoepidemiol Drug Saf. 2018. PMID: 30379372
-
Post percutaneous coronary interventional adverse cardiovascular outcomes and bleeding events observed with prasugrel versus clopidogrel: direct comparison through a meta-analysis.BMC Cardiovasc Disord. 2018 May 2;18(1):78. doi: 10.1186/s12872-018-0820-6. BMC Cardiovasc Disord. 2018. PMID: 29720092 Free PMC article. Review.
-
Prasugrel or ticagrelor relative to clopidogrel in triple-antiplatelet treatment combined with glycoprotein IIb/IIIa inhibitor for patients with STEMI undergoing PCI: a meta-analysis.BMC Cardiovasc Disord. 2020 Mar 12;20(1):130. doi: 10.1186/s12872-020-01403-6. BMC Cardiovasc Disord. 2020. PMID: 32164560 Free PMC article.
Cited by
-
Prognostic impact of the atherogenic index of plasma in type 2 diabetes mellitus patients with acute coronary syndrome undergoing percutaneous coronary intervention.Lipids Health Dis. 2020 Nov 16;19(1):240. doi: 10.1186/s12944-020-01418-0. Lipids Health Dis. 2020. PMID: 33198752 Free PMC article.
-
Ticagrelor versus Clopidogrel in Patients with Severe Renal Insufficiency Undergoing PCI for Acute Coronary Syndrome.J Interv Cardiol. 2022 Jul 31;2022:6476777. doi: 10.1155/2022/6476777. eCollection 2022. J Interv Cardiol. 2022. PMID: 35966043 Free PMC article.
-
Comparison of 1-Year Clinical Outcomes Between Ticagrelor Versus Clopidogrel in Type 2 Diabetes Patients After Implantation of Small Diameter Stents.Anatol J Cardiol. 2025 Jan 7;29(2):95-103. doi: 10.14744/AnatolJCardiol.2024.4603. Online ahead of print. Anatol J Cardiol. 2025. PMID: 39763313 Free PMC article.
-
Cardiovascular Outcomes Observed with Ticagrelor versus Clopidogrel in Type 2 Diabetes Mellitus Patients with Acute Coronary Syndrome: A Meta-analysis.Diabetes Ther. 2023 Feb;14(2):387-399. doi: 10.1007/s13300-022-01354-5. Epub 2022 Dec 21. Diabetes Ther. 2023. PMID: 36542307 Free PMC article.
-
Risk of Bleeding and Ischemia in Elderly East Asian Patients with Diabetes Mellitus Treated with either Clopidogrel or Ticagrelor: From the Korean Acute Myocardial Infarction Registry-V.Chonnam Med J. 2024 Sep;60(3):147-154. doi: 10.4068/cmj.2024.60.3.147. Epub 2024 Sep 25. Chonnam Med J. 2024. PMID: 39381120 Free PMC article.
References
-
- Roffi M, Patrono C, Collet J-P, et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: task force for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation of the European society of cardiology (ESC). Eur Heart J 2016;37:267–315. - PubMed
-
- Levine GN, Bates ER, Bittl JA, et al. 2016 ACC/AHA guideline focused update on duration of dual antiplatelet therapy in patients with coronary artery disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Thorac Cardiovasc Surg 2016;152:1243–75. - PubMed
-
- Antman EM, Wiviott SD, Murphy SA, et al. Early and late benefits of prasugrel in patients with acute coronary syndromes undergoing percutaneous coronary intervention: a TRITON–TIMI 38 (TRial to assess improvement in therapeutic outcomes by optimizing platelet inhibition with prasugrel–thrombolysis in myocardial infarction) analysis. J Am Coll Cardiol 2008;51:2028–33. - PubMed
-
- Becker RC, Bassand JP, Budaj A, et al. Bleeding complications with the P2Y12 receptor antagonists clopidogrel and ticagrelor in the platelet inhibition and patient outcomes (PLATO) trial. Eur Heart J 2011;32:2933–44. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
