

Platelet reactivity patterns in patients treated with dual antiplatelet therapy
- PMID: 30882911
- PMCID: PMC6593782
- DOI: 10.1111/eci.13102
Platelet reactivity patterns in patients treated with dual antiplatelet therapy
Abstract
Aim: The aim of the present study was to investigate the patterns of platelet reactivity and discriminators of therapeutic response to dual antiplatelet therapy (DAPT) with aspirin and ticagrelor or prasugrel in patients with acute coronary syndrome (ACS).
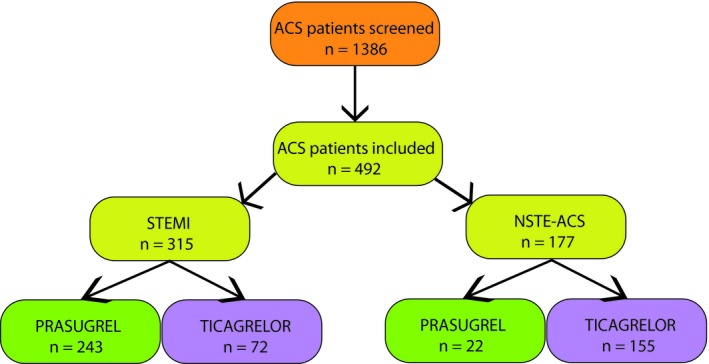
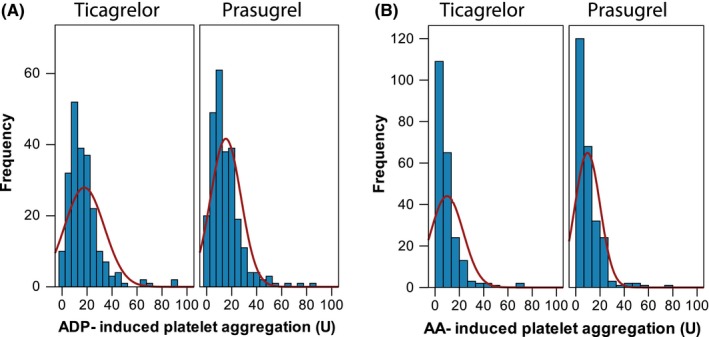
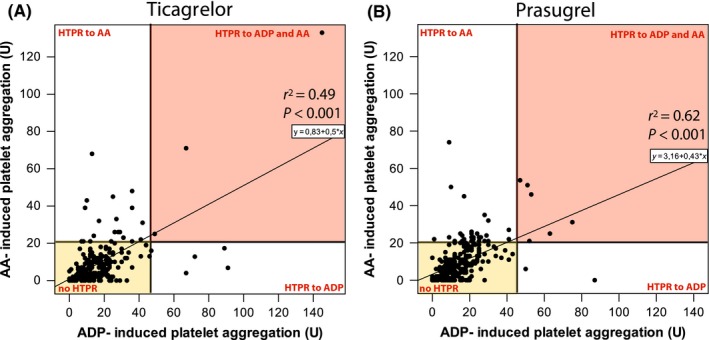
Design: In this multicentre prospective observational study, 492 patients with ACS were enrolled. Platelet aggregation was determined by multiple electrode aggregometry after stimulation with adenosine diphosphate (ADP) or arachidonic acid (AA) as agonists in the maintenance phase of treatment with prasugrel or ticagrelor.
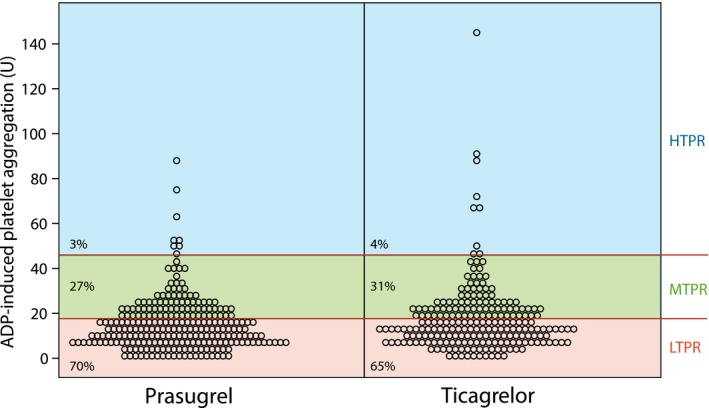
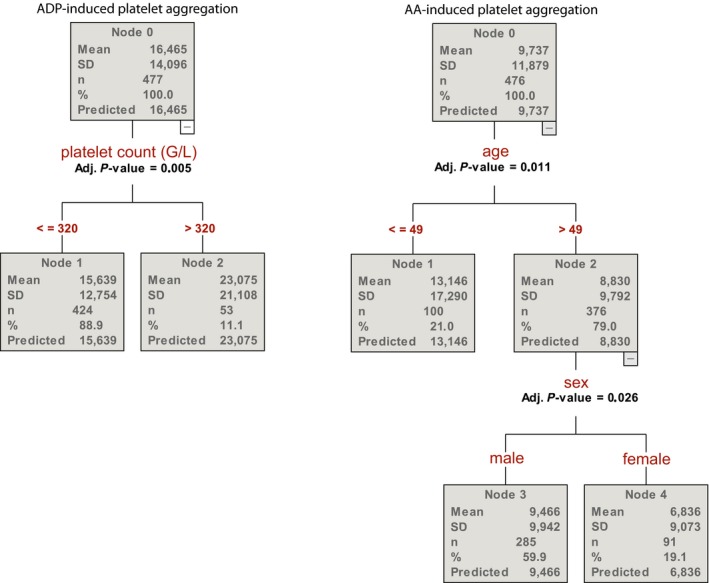
Results: Age emerged as the strongest variable influencing aspirin response status: The mean AA-induced platelet aggregation in patients <49 years of age was 49% higher than in those >49 years (13.1 U vs 8.8 U; P = 0.011). The second strongest discriminator of aspirin response was sex: Male patients had a 40% higher AA-induced platelet aggregation values than female patients (9.5 U vs 6.8 U; P = 0.026). Platelet count emerged as the only variable influencing ADP antagonists response status showing that patients with platelet count >320 g/L displayed higher ADP-induced platelet aggregation. About 12% of patients had high on-treatment platelet reactivity (HTPR) to aspirin, 3% and 4% a HTPR to prasugrel and ticagrelor, respectively, and only 2% displayed HTPR to dual antiplatelet therapy.
Conclusion: When potent platelet inhibitors as prasugrel and ticagrelor are administered with aspirin, HTPR to DAPT plays only a marginal role.
Keywords: ACS; HTPR; LTPR; MEA; platelets; prasugrel; ticagrelor.
© 2019 The Authors. European Journal of Clinical Investigation published by John Wiley & Sons Ltd on behalf of Stichting European Society for Clinical Investigation Journal Foundation.
Conflict of interest statement
DvL received honoraria for advisory boards from AstraZeneca and Daiichi Sankyo. JSM received lecture or consultant fees from Daaichi, Eli Lilly, Bayer, Roche and Astra Zeneca. All other authors report no conflict of interests.
Figures
Similar articles
-
Impact of Prasugrel and Ticagrelor on Platelet Reactivity in Patients With Acute Coronary Syndrome: A Meta-Analysis.Front Cardiovasc Med. 2022 Jun 9;9:905607. doi: 10.3389/fcvm.2022.905607. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35757353 Free PMC article.
-
Comparison of Light Transmission Aggregometry With Impedance Aggregometry in Patients on Potent P2Y12 Inhibitors.J Cardiovasc Pharmacol Ther. 2021 May;26(3):260-268. doi: 10.1177/1074248420968706. Epub 2020 Oct 27. J Cardiovasc Pharmacol Ther. 2021. PMID: 33107322 Free PMC article.
-
Inter-patient variability of platelet reactivity in patients treated with prasugrel and ticagrelor.Platelets. 2016 Jun;27(4):373-7. doi: 10.3109/09537104.2015.1095874. Epub 2015 Nov 10. Platelets. 2016. PMID: 26555925
-
Comparison of platelet reactivity between prasugrel and ticagrelor in patients with acute coronary syndrome: a meta-analysis.BMC Cardiovasc Disord. 2020 Oct 1;20(1):430. doi: 10.1186/s12872-020-01603-0. BMC Cardiovasc Disord. 2020. PMID: 33004000 Free PMC article.
-
Serum uric acid levels during dual antiplatelet therapy with ticagrelor or clopidogrel: Results from a single-centre study.Nutr Metab Cardiovasc Dis. 2016 Jul;26(7):567-574. doi: 10.1016/j.numecd.2016.03.001. Epub 2016 Mar 15. Nutr Metab Cardiovasc Dis. 2016. PMID: 27134063
Cited by
-
Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor Blockers in Acute Coronary Syndrome: Implications for Platelet Reactivity?Cardiovasc Drugs Ther. 2021 Dec;35(6):1183-1190. doi: 10.1007/s10557-020-07128-0. Epub 2020 Dec 18. Cardiovasc Drugs Ther. 2021. PMID: 33337519 Free PMC article.
-
Elevated High-Sensitivity C-Reactive Protein Level Enhances the Impact of Lipoprotein(a) on Platelet Reactivity in PCI Patients Treated with Clopidogrel.Clin Appl Thromb Hemost. 2024 Jan-Dec;30:10760296241280711. doi: 10.1177/10760296241280711. Clin Appl Thromb Hemost. 2024. PMID: 39246223 Free PMC article.
-
Impact of Prasugrel and Ticagrelor on Platelet Reactivity in Patients With Acute Coronary Syndrome: A Meta-Analysis.Front Cardiovasc Med. 2022 Jun 9;9:905607. doi: 10.3389/fcvm.2022.905607. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35757353 Free PMC article.
-
High-Intensity Exercise Training Improves Basal Platelet Prostacyclin Sensitivity and Potentiates the Response to Dual Anti-Platelet Therapy in Postmenopausal Women.Biomolecules. 2022 Oct 17;12(10):1501. doi: 10.3390/biom12101501. Biomolecules. 2022. PMID: 36291709 Free PMC article.
-
The Effectiveness of Antiplatelet Therapy and the Factors Influencing It in Patients with Acute Coronary Syndrome before and during the COVID-19 Pandemic.Medicina (Kaunas). 2022 Dec 30;59(1):84. doi: 10.3390/medicina59010084. Medicina (Kaunas). 2022. PMID: 36676708 Free PMC article.
References
-
- Cuisset T, Deharo P, Quilici J, et al. Benefit of switching dual antiplatelet therapy after acute coronary syndrome: the TOPIC (timing of platelet inhibition after acute coronary syndrome) randomized study. Eur Heart J. 2017;38(41):3070‐3078. - PubMed
-
- Winter M‐P, Grove EL, De Caterina R, et al. Advocating cardiovascular precision medicine with P2Y12 receptor inhibitors. Eur Heart J Cardiovasc Pharmacother. 2017;3(4):221‐234. - PubMed
-
- Wiviott SD, Braunwald E, McCabe CH, et al. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N Engl J Med. 2007;357(20):2001‐2015. - PubMed
-
- Wallentin L, Becker RC, Budaj A, et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N Engl J Med. 2009;361(11):1045‐1057. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
