

Comparing phase and electrographic flow mapping for persistent atrial fibrillation
- PMID: 30882924
- PMCID: PMC6476687
- DOI: 10.1111/pace.13649
Comparing phase and electrographic flow mapping for persistent atrial fibrillation
Abstract
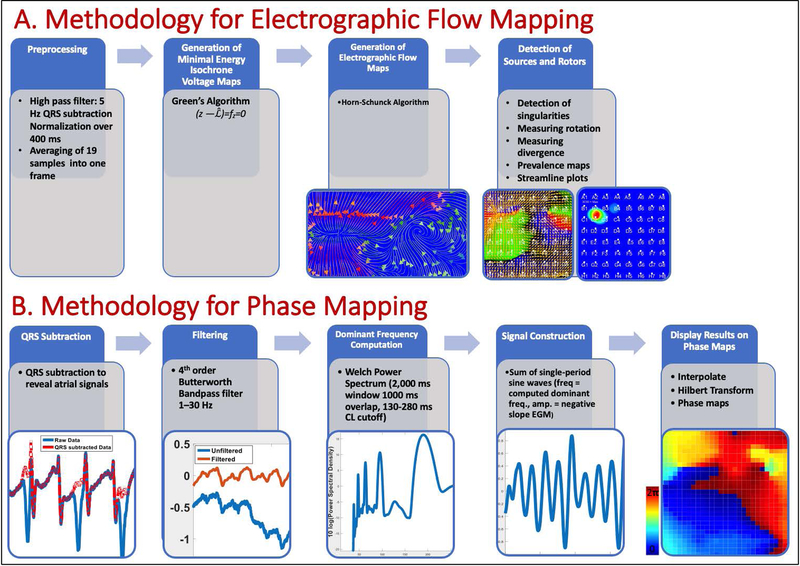
Background: An increasing number of methods are being used to map atrial fibrillation (AF), yet the sensitivity of identifying potential localized AF sources of these novel methods are unclear. Here, we report a comparison of two approaches to map AF based upon (1) electrographic flow mapping and (2) phase mapping in a multicenter registry of patients in whom ablation terminated persistent AF.
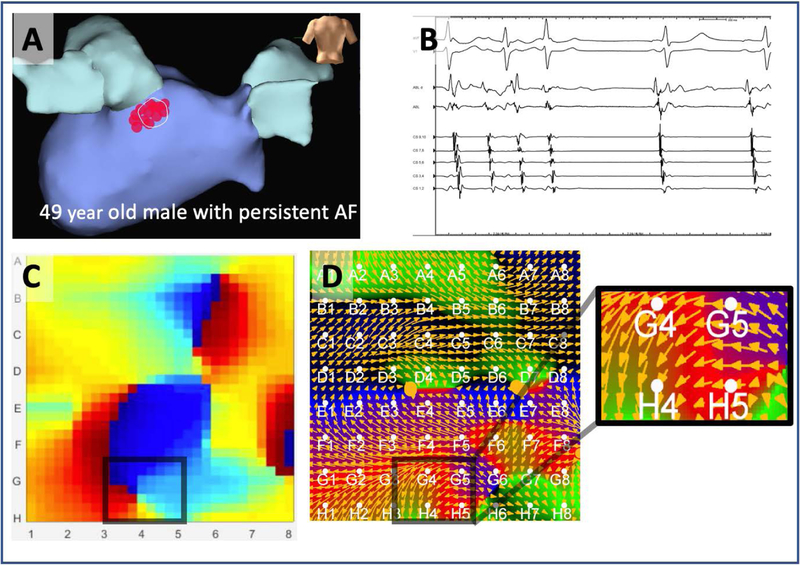
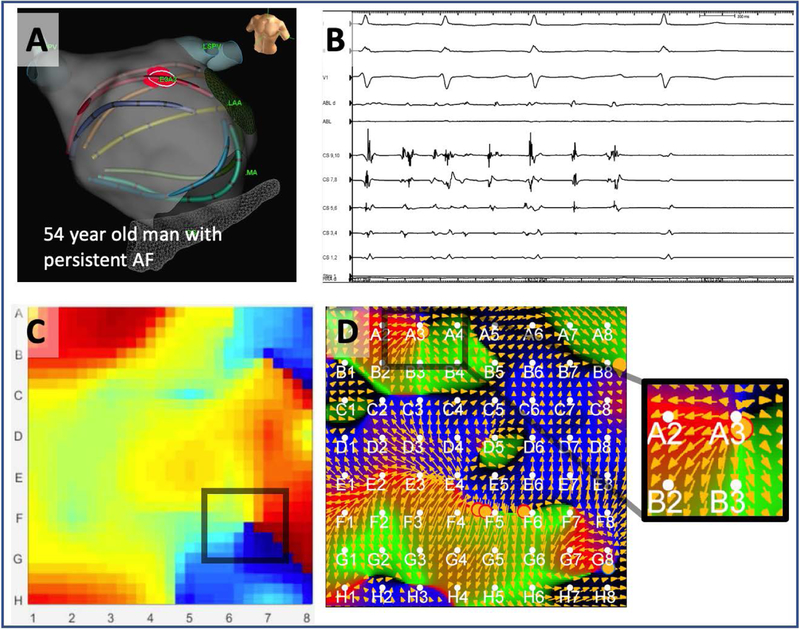
Methods: Fifty-three consecutive patients with persistent AF in whom ablation terminated AF in an international multicenter registry were enrolled. Electrographic flow mapping (EGF) and phase mapping were applied to the multipolar simultaneous electrograms recorded from a 64-pole basket catheter in the chamber (left vs right atrium) where AF termination occurred. We analyzed if the mapping methods were able to detect localized sources at the AF termination site. We also analyzed global results of mapping AF for each method, patterns of activation of localized sources.
Results: Patients were 64.3 ± 9.4 years old and 69.8% were male. EGF and phase mapping identified localized sources at AF termination sites in 81% and 83% of the patients, respectively. Methods were complementary and in only n = 2 (3.7%) neither method identified a source. Globally, EGF identified more localized sources than phase mapping (5.3 ± 2.8 vs 1.8 ± 0.5, P < 0.001), with a higher prevalence of focal (compared to rotational) activation pattern (49% vs 2%, P < 0.01).
Conclusions: EGF is a novel vectorial-based AF mapping method, which can detect sites of AF termination, agreeing with, and complementary to, an alternative AF mapping method using phase analysis.
Keywords: atrial fibrillation; electrographic flow; electrophysiology; mapping; phase.
© 2019 Wiley Periodicals, Inc.
Figures

References
-
- Verma A, Jiang C-Y, Betts TR, Chen J, Deisenhofer I, Mantovan R, Macle L, Morillo C a, Haverkamp W, Weerasooriya R, Albenque J-P, Nardi S, Menardi E, Novak P, Sanders P. Approaches to Catheter Ablation for Persistent Atrial Fibrillation. NEJM 2015; 372:1812–1822. - PubMed
-
- Ramirez FD, Birnie DH, Nair GM, Szczotka A, Redpath CJ, Sadek MM, Nery PB. Efficacy and safety of driver-guided catheter ablation for atrial fibrillation: A systematic review and meta-analysis. JCE 2017; 28:1371–1378. - PubMed
-
- Umapathy K, Nair K, Masse S, Krishnan S, Rogers J, Nash MP, Nanthakumar K. Phase mapping of cardiac fibrillation. Circ: AE 2010; 3:105–114. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
