

A Formula for Estimating the Appropriate Tube Depth for Intubation
- PMID: 30883238
- PMCID: PMC6424171
- DOI: 10.2344/anpr-65-04-04
A Formula for Estimating the Appropriate Tube Depth for Intubation
Abstract
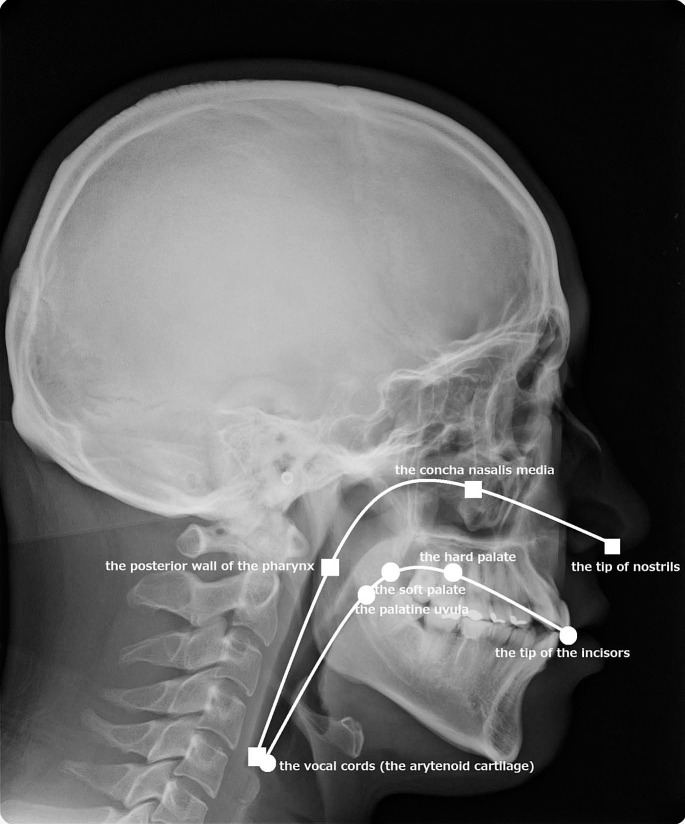
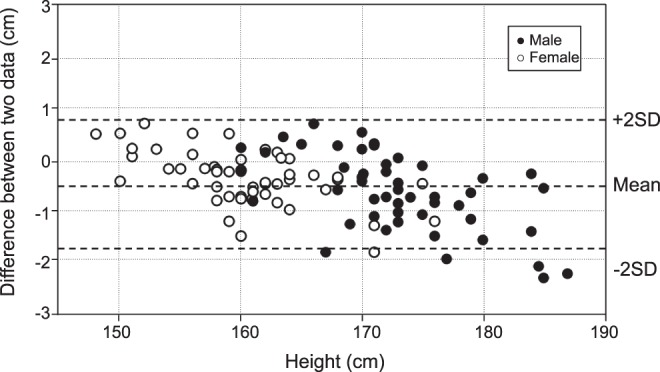
An estimation of the appropriate tubing depth for fixation is helpful to prevent inadvertent endobronchial intubation and prolapse of cuff from the vocal cord. A feasible estimation formula should be established. We measured the anatomical length of the upper-airway tract through the oral and nasal pathways on cephalometric radiographs and tried to establish the estimation formula from the height of the patient. The oral upper-airway tract was measured from the tip of the incisor to the vocal cord. The nasal upper-airway tract was measured from the tip of the nostril to the vocal cord. The tracts were smoothly traced by using software. The length of the oral upper-airway tract was 13.2 ± 0.8 cm, and the nasal upper-airway tract was 16.1 ± 0.9 cm. We found no gender difference ( p > .05). The correlations between the patients' height and the length of the oral and nasal upper-airway tracts were 0.692 and 0.760, respectively. We found that the formulas (height/10) - 3 (in cm) for oral upper-airway and (height/10) + 1 (in cm) for nasal upper-airway tract are the simple fit estimation formulas. The average error and standard deviation of the estimated values from the measured values were 0.50 ± 0.66 cm for the oral tract and 0.39 ± 0.63 cm for the nasal tract. Thus, considering the length of the intubation marker of each product (DM), we would like to propose the length of tube fixation as (height/10) + 1 + DM for nasal intubation and (height/10) - 3 + DM for oral intubation. In conclusion, the estimation formulas of (height/10) - 3 + DM and (height/10) + 1 + DM for oral and nasal intubation, respectively, are within almost 1 cm error in most cases.
Keywords: Cephalogram; General anesthesia; Intubation tube; Larynx; Nasal intubation; Oral intubation; Tracheal.
Figures




References
-
- Caplan RA, Posner KL, Ward RJ, Cheney FW. Adverse respiratory events in anesthesia: a closed claims analysis. Anesthesiology. 1990;72:828–833. - PubMed
-
- Ramsingh D, Frank E, Haughton R, et al. Auscultation versus point-of-care ultrasound to determine endotracheal versus bronchial intubation: a diagnostic accuracy study. Anesthesiology. 2016;124:1012–1020. - PubMed
-
- Dronen S, Chadwick O, Nowak R. Endotracheal tip position in the arrested patient. Ann Emerg Med. 1982;11:116–117. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
