

Randomized controlled comparison of cross-sectional survey approaches to optimize follow-up completeness in clinical studies
- PMID: 30883589
- PMCID: PMC6422260
- DOI: 10.1371/journal.pone.0213822
Randomized controlled comparison of cross-sectional survey approaches to optimize follow-up completeness in clinical studies
Abstract
Introduction: In outcome research, incomplete follow-up is a major, yet potentially correctable source of bias. Cross-sectional surveys may theoretically increase completeness of follow-up, but low response rates are reported typically. We investigated whether a pre-notification letter improved patient availability for follow-up phone interviews and thereby improved cross-sectional survey yield.
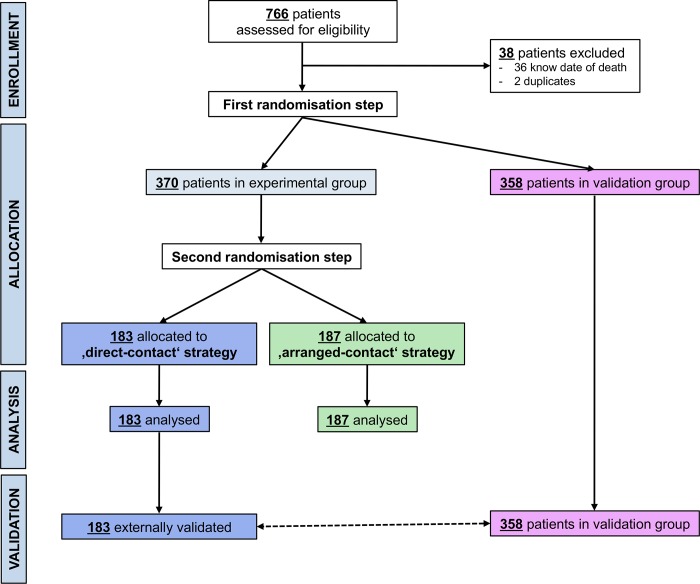
Methods: A consecutive series of vascular patients was randomly divided into a trial and a validation population. The trial population was then randomized 1:1 to one of two cross-sectional contact strategies: Strategy 1 consisted of direct contact attempts by up to 12 systematically timed phone calls, whereas Strategy 2 used a personalized pre-notification letter to arrange for scheduled phone call interviews. Response rates, average time and efforts needed per patient and overall survey duration were compared. Subsequently, trial findings were externally validated in the validation population.
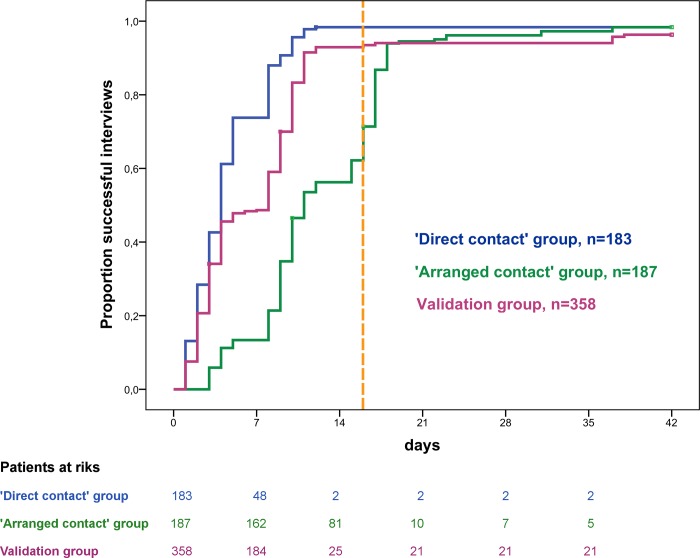
Results: Of 728 consecutive patients, 370 were allocated to the trial population. Trial patients contacted by strategy 1 (n = 183) had a similar profile when compared to trial patients contacted by strategy 2 (n = 187). Follow-up periods following surgery (54.3 versus 53.6 months) and all-cause mortality rates (21.3% versus 18.7%) were comparable between the trial groups. Cross-sectional information on survival outcomes was almost complete after both contact strategies (99.5% versus 98.9%, P = 1.0). In 144/187 strategy 2 patients (77%) interviews were scheduled successfully necessitating significantly less contact attempts (median of 1.3 versus 2.3 per patient, P<0.0001). However, invested time per patient was similar between the groups (median of 10.1 versus 9.6 minutes), and survey strategy 1 completed earlier (median time to contact 4 versus 11 days, P<0.0001). Therefore, strategy 1 was validated in the validation population (n = 358): a low lost to follow-up rate below 1% (P = 1.0) was reconfirmed necessitating an average of 2.3 contact attempts per patient.
Conclusions: Both contact strategies were equally successful in contacting almost all patients cross-sectionally. If systematically timed, direct phone calls were less complicated to organize and faster completed. Given the low time and effort per patient, outcome studies should invest in systematic follow-up surveys to minimize attrition bias.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Clark TG, Altman DG, De Stavola BL. Quantification of the completeness of follow-up. Lancet. 2002;359(9314):1309–10. . - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
