

Combining quick sequential organ failure assessment score with heart rate variability may improve predictive ability for mortality in septic patients at the emergency department
- PMID: 30883595
- PMCID: PMC6422271
- DOI: 10.1371/journal.pone.0213445
Combining quick sequential organ failure assessment score with heart rate variability may improve predictive ability for mortality in septic patients at the emergency department
Abstract
Background: Although the quick Sequential Organ Failure Assessment (qSOFA) score was recently introduced to identify patients with suspected infection/sepsis, it has limitations as a predictive tool for adverse outcomes. We hypothesized that combining qSOFA score with heart rate variability (HRV) variables improves predictive ability for mortality in septic patients at the emergency department (ED).
Methods: This was a retrospective study using the electronic medical record of a tertiary care hospital in Singapore between September 2014 and February 2017. All patients aged 21 years or older who were suspected with infection/sepsis in the ED and received electrocardiography monitoring with ZOLL X Series Monitor (ZOLL Medical Corporation, Chelmsford, MA) were included. We fitted a logistic regression model to predict the 30-day mortality using one of the HRV variables selected from one of each three domains those previously reported as strong association with mortality (i.e. standard deviation of NN [SDNN], ratio of low frequency to high frequency power [LF/HF], detrended fluctuation analysis α-2 [DFA α-2]) in addition to the qSOFA score. The predictive accuracy was assessed with other scoring systems (i.e. qSOFA alone, National Early Warning Score, and Modified Early Warning Score) using the area under the receiver operating characteristic curve.
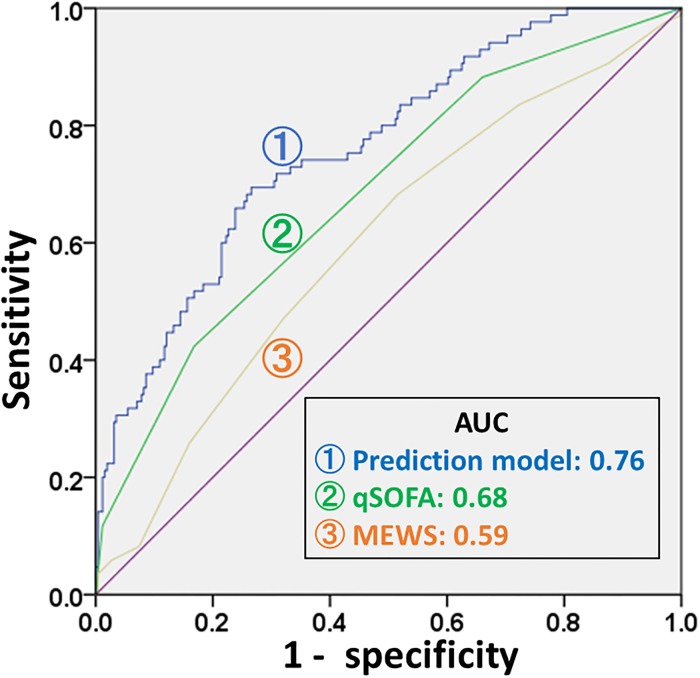
Results: A total of 343 septic patients were included. Non-survivors were significantly older (survivors vs. non-survivors, 65.7 vs. 72.9, p <0.01) and had higher qSOFA (0.8 vs. 1.4, p <0.01) as compared to survivors. There were significant differences in HRV variables between survivors and non-survivors including SDNN (23.7s vs. 31.8s, p = 0.02), LF/HF (2.8 vs. 1.5, p = 0.02), DFA α-2 (1.0 vs. 0.7, P < 0.01). Our prediction model using DFA-α-2 had the highest c-statistic of 0.76 (95% CI, 0.70 to 0.82), followed by qSOFA of 0.68 (95% CI, 0.62 to 0.75), National Early Warning Score at 0.67 (95% CI, 0.61 to 0.74), and Modified Early Warning Score at 0.59 (95% CI, 0.53 to 0.67).
Conclusions: Adding DFA-α-2 to the qSOFA score may improve the accuracy of predicting in-hospital mortality in septic patients who present to the ED. Further multicenter prospective studies are required to confirm our results.
Conflict of interest statement
NL and MO have a patent filing that is not directly related to this study (System and method of determining a risk score for triage, Application Number: US 13/791,764). MO has a similar patent filing unrelated to this study (Method of predicting acute cardiopulmonary events and survivability of a patient, Application Number: US 13/047,348). MO also has a licensing agreement with ZOLL Medical Corporation for the above patented technology. There are no further patents, products in development or marketed products to declare. All the other authors do not have either commercial or personal associations or any sources of support that might pose a conflict of interest in the subject matter or materials discussed in this manuscript. Our conflict of interest does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
