

What Words Convey: The Potential for Patient Narratives to Inform Quality Improvement
- PMID: 30883954
- PMCID: PMC6422610
- DOI: 10.1111/1468-0009.12374
What Words Convey: The Potential for Patient Narratives to Inform Quality Improvement
Abstract
Policy Points Narratives about patients' experiences with outpatient care are essential for quality improvement because they convey ample actionable information that both elaborates on existing domains within patient experience surveys and describes multiple additional domains that are important to patients. The content of narrative feedback from patients can potentially be translated to improved quality in multiple ways: clinicians can learn from their own patients, groups of clinicians can learn from the experience of their peers' patients, and health system administrators can identify and respond to patterns in patients' accounts that reflect systemic challenges to quality. Consistent investment by payers and providers is required to ensure that patient narratives are rigorously collected, analyzed fully, and effectively used for quality improvement.
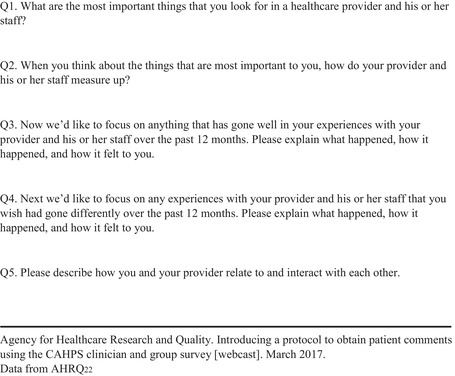
Context: For the past 25 years, health care providers and health system administrators have sought to improve care by surveying patients about their experiences. More recently, policymakers have acted to promote this learning by deploying financial incentives tied to survey scores. This article explores the potential of systematically elicited narratives about experiences with outpatient care to enrich quality improvement.
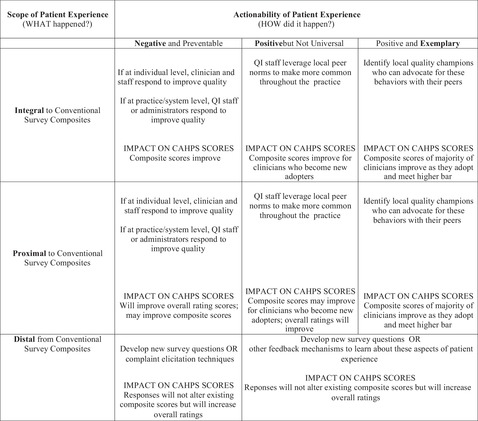
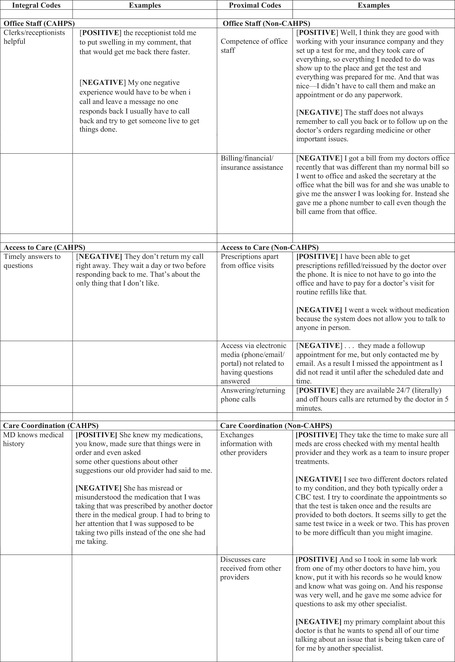
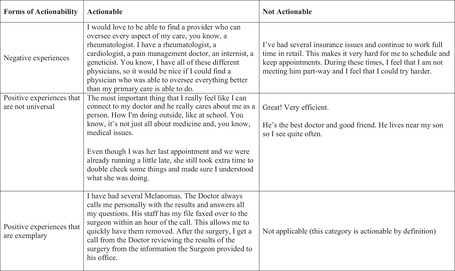
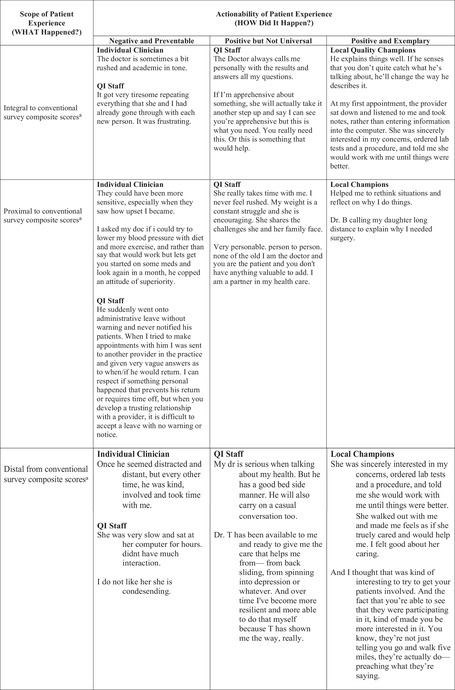
Methods: Narratives were collected from 348 patients recruited from a nationally representative Internet panel. Drawing from the literature on health services innovation, we developed a two-part coding schema that categorized narrative content in terms of (a) the aspects of care being described, and (b) the actionability of this information for clinicians, quality improvement staff, and health system administrators. Narratives were coded using this schema, with high levels of reliability among the coders.
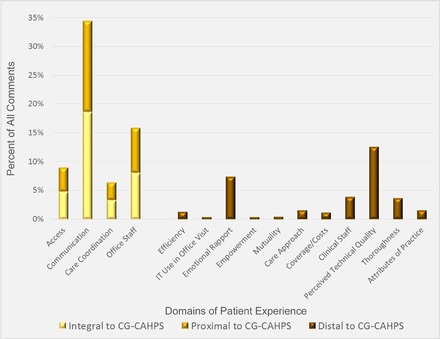
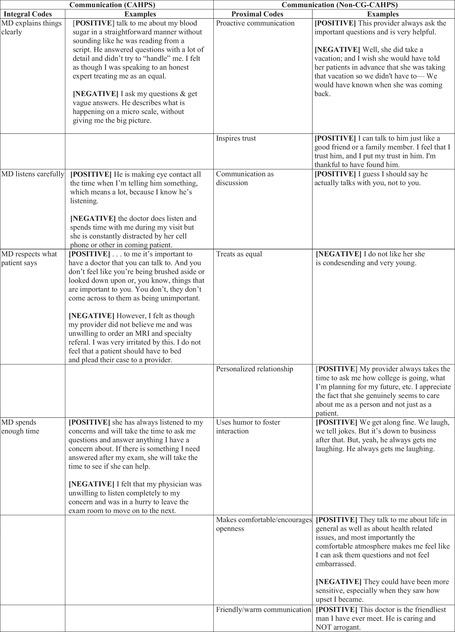
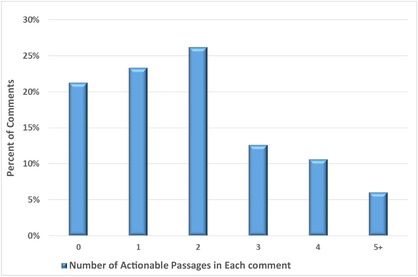
Findings: The scope of outpatient narratives divides evenly among aspects of care currently measured by patient experience surveys (35% of content), aspects related to measured domains but not captured by existing survey questions (31%), and aspects of care that are omitted from surveys entirely (34%). Overall, the narrative data focused heavily on relational aspects of care (43%), elaborating on this aspect of experience well beyond what is captured with communication-related questions on existing surveys. Three-quarters of elicited narratives had some actionable content, and almost a third contained three or more separate actionable elements.
Conclusions: In a health policy environment that incentivizes attention to patient experience, rigorously elicited narratives hold substantial promise for improving quality in general and patients' experiences with care in particular. They do so in two ways: by making concrete what went wrong or right in domains covered by existing surveys, and by expanding our view of what aspects of care matter to patients as articulated in their own words and thus how care can be made more patient-centered. Most narratives convey experiences that are potentially actionable by those committed to improving health care quality in outpatient settings.
Keywords: narratives; patient experience; patient surveys; patient-centered; quality improvement.
© 2019 Milbank Memorial Fund.
Figures

Similar articles
-
Sexual Harassment and Prevention Training.2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 36508513 Free Books & Documents.
-
Access Points: Understanding Special Interests Through Autistic Narratives.Autism Adulthood. 2025 Feb 5;7(1):100-111. doi: 10.1089/aut.2023.0157. eCollection 2025 Feb. Autism Adulthood. 2025. PMID: 40151658
-
"In a State of Flow": A Qualitative Examination of Autistic Adults' Phenomenological Experiences of Task Immersion.Autism Adulthood. 2024 Sep 16;6(3):362-373. doi: 10.1089/aut.2023.0032. eCollection 2024 Sep. Autism Adulthood. 2024. PMID: 39371355
-
The Lived Experience of Autistic Adults in Employment: A Systematic Search and Synthesis.Autism Adulthood. 2024 Dec 2;6(4):495-509. doi: 10.1089/aut.2022.0114. eCollection 2024 Dec. Autism Adulthood. 2024. PMID: 40018061 Review.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of paclitaxel, docetaxel, gemcitabine and vinorelbine in non-small-cell lung cancer.Health Technol Assess. 2001;5(32):1-195. doi: 10.3310/hta5320. Health Technol Assess. 2001. PMID: 12065068
Cited by
-
Integration of patient and clinician narratives into systematic reviews: An applied proof of concept.J Clin Transl Sci. 2021 Jan 19;5(1):e78. doi: 10.1017/cts.2021.2. J Clin Transl Sci. 2021. PMID: 34007463 Free PMC article.
-
Exploring the Impact of Storytelling for Hospitalized Patients Recovering from COVID-19.Healthcare (Basel). 2023 Feb 16;11(4):589. doi: 10.3390/healthcare11040589. Healthcare (Basel). 2023. PMID: 36833123 Free PMC article.
-
Social determinants of ambulatory care sensitive conditions: a qualitative meta-synthesis based on patient perspectives.Front Public Health. 2023 May 9;11:1147732. doi: 10.3389/fpubh.2023.1147732. eCollection 2023. Front Public Health. 2023. PMID: 37228726 Free PMC article.
-
Family Input for Quality and Safety (FIQS): Using mobile technology for in-hospital reporting from families and patients.J Hosp Med. 2022 Jun;17(6):456-465. doi: 10.1002/jhm.2777. Epub 2022 Feb 4. J Hosp Med. 2022. PMID: 35535946 Free PMC article.
-
Learning from patients: The impact of using patients' narratives on patient experience scores.Health Care Manage Rev. 2024 Jan-Mar 01;49(1):2-13. doi: 10.1097/HMR.0000000000000386. Health Care Manage Rev. 2024. PMID: 38019459 Free PMC article.
References
-
- Grob R. The heart of patient‐centered care. J Health Polit Policy Law. 2013;38(2):457‐465. - PubMed
-
- Tanenbaum SJ. What is patient‐centered care? A typology of models and missions. Health Care Anal. 2015;23(3):272‐287. - PubMed
-
- Frampton SB, Guastello S, Hoy L, Naylor M, Sheridan S, Johnston‐Fleece M. Harnessing evidence and experience to change culture: a guiding framework for patient and family engaged care. Discussion Paper (January 31, 2017), National Academy of Medicine, Washington, DC. https://nam.edu/wp-content/uploads/2017/01/Harnessing-Evidence-and-Exper.... Accessed February 12, 2019.
-
- Crofton C, Lubalin JS, Darby C. Foreword. Consumer Assessment of Health Plans Study (CAHPS). Med Care. 1999;37(Suppl. 3):MS1‐9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
