

Service Delivery Models to Maximize Quality of Life for Older People at the End of Life: A Rapid Review
- PMID: 30883956
- PMCID: PMC6422603
- DOI: 10.1111/1468-0009.12373
Service Delivery Models to Maximize Quality of Life for Older People at the End of Life: A Rapid Review
Abstract
Policy Points We identified two overarching classifications of integrated geriatric and palliative care to maximize older people's quality of life at the end of life. Both are oriented to person-centered care, but with differing emphasis on either function or symptoms and concerns. Policymakers should both improve access to palliative care beyond just the last months of life and increase geriatric care provision to maintain and optimize function. This would ensure that continuity and coordination for potentially complex care needs across the continuum of late life would be maintained, where the demarcation of boundaries between healthy aging and healthy dying become increasingly blurred. Our findings highlight the urgent need for health system change to improve end-of-life care as part of universal health coverage. The use of health services should be informed by the likelihood of benefits and intended outcomes rather than on prognosis.
Context: In an era of unprecedented global aging, a key priority is to align health and social services for older populations in order to support the dual priorities of living well while adapting to a gradual decline in function. We aimed to provide a comprehensive synthesis of evidence regarding service delivery models that optimize the quality of life (QoL) for older people at the end of life across health, social, and welfare services worldwide.
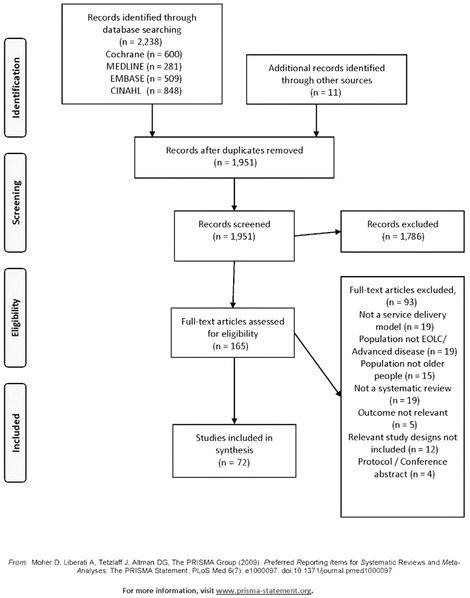
Methods: We conducted a rapid scoping review of systematic reviews. We searched MEDLINE, CINAHL, EMBASE, and CDSR databases from 2000 to 2017 for reviews reporting the effectiveness of service models aimed at optimizing QoL for older people, more than 50% of whom were older than 60 and in the last one or two years of life. We assessed the quality of these included reviews using AMSTAR and synthesized the findings narratively.
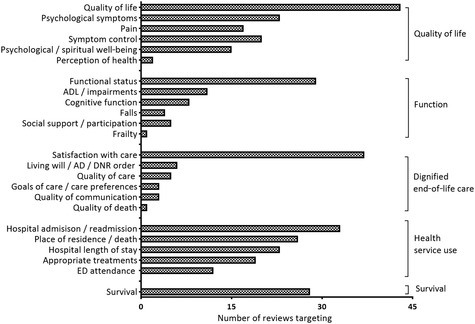
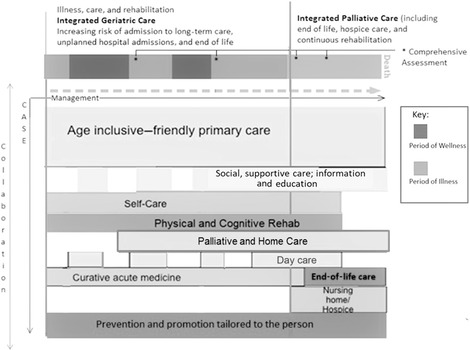
Results: Of the 2,238 reviews identified, we included 72, with 20 reporting meta-analysis. Although all the World Health Organization (WHO) regions were represented, most of the reviews reported data from the Americas (52 of 72), Europe (46 of 72), and/or the Western Pacific (28 of 72). We identified two overarching classifications of service models but with different target outcomes: Integrated Geriatric Care, emphasizing physical function, and Integrated Palliative Care, focusing mainly on symptoms and concerns. Areas of synergy across the overarching classifications included person-centered care, education, and a multiprofessional workforce. The reviews assessed 117 separate outcomes. A meta-analysis demonstrated effectiveness for both classifications on QoL, including symptoms such as pain, depression, and psychological well-being. Economic analysis and its implications were poorly considered.
Conclusions: Despite their different target outcomes, those service models classified as Integrated Geriatric Care or Integrated Palliative Care were effective in improving QoL for older people nearing the end of life. Both approaches highlight the imperative for integrating services across the care continuum, with service involvement triggered by the patient's needs and likelihood of benefits. To inform the sustainability of health system change we encourage economic analyses that span health and social care and examine all sources of finance to understand contextual inequalities.
Keywords: geriatrics; health services for the aged; palliative care; quality of life.
© 2019 The Authors The Milbank Quarterly published by Wiley Periodicals, Inc. on behalf of The Millbank Memorial Fund.
Figures
References
-
- World Health Organization . World Report on Ageing and Health. Geneva, Switzerland: World Health Organization; 2015.
-
- Nicholson C, Meyer J, Flatley M, Holman C, Lowton K. Living on the margin: understanding the experience of living and dying with frailty in old age. Soc Sci Med. 2012;75(8):1426‐1432. - PubMed
-
- Moens K, Higginson IJ, Harding R, Euro I. Are there differences in the prevalence of palliative care‐related problems in people living with advanced cancer and eight non‐cancer conditions? A systematic review. J Pain Symptom Manage. 2014;48(4):660‐677. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
