

Learning From History About Reducing Infant Mortality: Contrasting the Centrality of Structural Interventions to Early 20th-Century Successes in the United States to Their Neglect in Current Global Initiatives
- PMID: 30883959
- PMCID: PMC6422600
- DOI: 10.1111/1468-0009.12376
Learning From History About Reducing Infant Mortality: Contrasting the Centrality of Structural Interventions to Early 20th-Century Successes in the United States to Their Neglect in Current Global Initiatives
Abstract
Policy Points Current efforts to reduce infant mortality and improve infant health in low- and middle-income countries (LMICs) can benefit from awareness of the history of successful early 20th-century initiatives to reduce infant mortality in high-income countries, which occurred before widespread use of vaccination and medical technologies. Improvements in sanitation, civil registration, milk purification, and institutional structures to monitor and reduce infant mortality played a crucial role in the decline in infant mortality seen in the United States in the early 1900s. The commitment to sanitation and civil registration has not been fulfilled in many LMICs. Structural investments in sanitation and water purification as well as in civil registration systems should be central, not peripheral, to the goal of infant mortality reduction in LMICs.
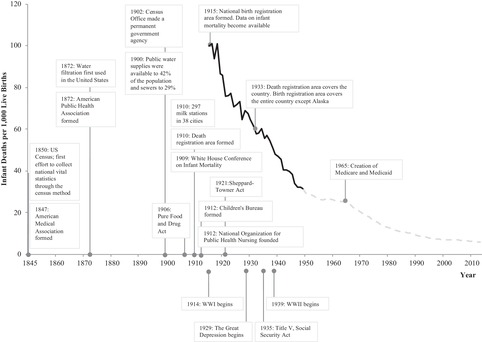
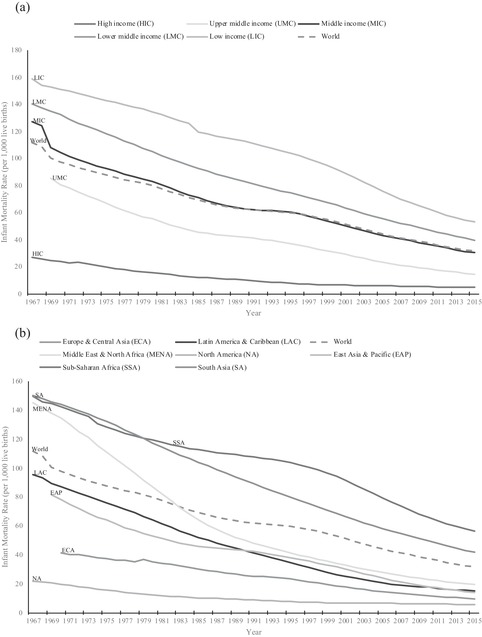
Context: Between 1915 and 1950, the infant mortality rate (IMR) in the United States declined from 100 to fewer than 30 deaths per 1,000 live births, prior to the widespread use of medical technologies and vaccination. In 2015 the IMR in low- and middle-income countries (LMICs) was 53.2 deaths per 1,000 live births, which is comparable to the United States in 1935 when IMR was 55.7 deaths per 1,000 live births. We contrast the role of public health institutions and interventions for IMR reduction in past versus present efforts to reduce infant mortality in LMICs to critically examine the current evidence base for reducing infant mortality and to propose ways in which lessons from history can inform efforts to address the current burden of infant mortality.
Methods: We searched the peer-reviewed and gray literature on the causes and explanations behind the decline in infant mortality in the United States between 1850 and 1950 and in LMICs after 2000. We included historical analyses, empirical research, policy documents, and global strategies. For each key source, we assessed the factors considered by their authors to be salient in reducing infant mortality.
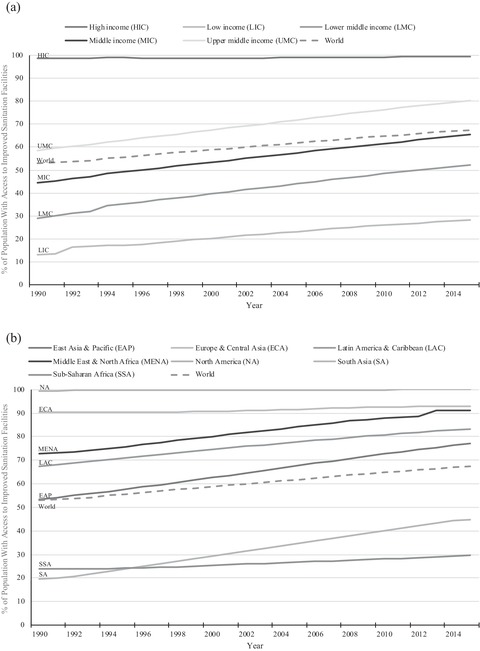
Findings: Public health programs that played a central role in the decline in infant mortality in the United States in the early 1900s emphasized large structural interventions like filtering and chlorinating water supplies, building sanitation systems, developing the birth and death registration area, pasteurizing milk, and also educating mothers on infant care and hygiene. The creation of new institutions and policies for infant health additionally provided technical expertise, mobilized resources, and engaged women's groups and public health professionals. In contrast, contemporary literature and global policy documents on reducing infant mortality in LMICs have primarily focused on interventions at the individual, household, and health facility level, and on the widespread adoption of cheap, ostensibly accessible, and simple technologies, often at the cost of leaving the structural conditions that determine child survival largely untouched.
Conclusions: Current discourses on infant mortality are not informed by lessons from history. Although structural interventions were central to the decline in infant mortality in the United States, current interventions in LMICs that receive the most global endorsement do not address these structural determinants of infant mortality. Using a historical lens to examine the continued problem of infant mortality in LMICs suggests that structural interventions, especially regarding sanitation and civil registration, should again become core to a public health approach to addressing infant mortality.
Keywords: civil registration and vital statistics (CRVS); history; infant mortality; low- and middle-income countries; sanitation.
© 2019 Milbank Memorial Fund.
Figures
Similar articles
-
The future of Cochrane Neonatal.Early Hum Dev. 2020 Nov;150:105191. doi: 10.1016/j.earlhumdev.2020.105191. Epub 2020 Sep 12. Early Hum Dev. 2020. PMID: 33036834
-
Mortality in a rural South African mission, 1837-1909: an historical cohort study using church records.Int J Epidemiol. 1993 Dec;22(6):965-75. doi: 10.1093/ije/22.6.965. Int J Epidemiol. 1993. PMID: 8144309
-
Socioeconomic development, health interventions and mortality decline in Costa Rica.Scand J Soc Med Suppl. 1991;46:33-42. Scand J Soc Med Suppl. 1991. PMID: 1805367
-
Schools of public health in low and middle-income countries: an imperative investment for improving the health of populations?BMC Public Health. 2016 Sep 7;16:941. doi: 10.1186/s12889-016-3616-6. BMC Public Health. 2016. PMID: 27604901 Free PMC article. Review.
-
Associations of women's empowerment with neonatal, infant and under-5 mortality in low- and /middle-income countries: meta-analysis of individual participant data from 59 countries.BMJ Glob Health. 2020 Jan 9;5(1):e001558. doi: 10.1136/bmjgh-2019-001558. eCollection 2020. BMJ Glob Health. 2020. PMID: 32133162 Free PMC article.
Cited by
-
The Political Realignment of Health: How Partisan Power Shaped Infant Health in the United States, 1915-2017.J Health Polit Policy Law. 2022 Apr 1;47(2):201-224. doi: 10.1215/03616878-9517191. J Health Polit Policy Law. 2022. PMID: 34522959 Free PMC article.
-
The foreign gaze: authorship in academic global health.BMJ Glob Health. 2019 Oct 18;4(5):e002068. doi: 10.1136/bmjgh-2019-002068. eCollection 2019. BMJ Glob Health. 2019. PMID: 31750005 Free PMC article. No abstract available.
-
Trends in Life Expectancy: Learning From International Comparisons.Am J Public Health. 2023 Sep;113(9):954-955. doi: 10.2105/AJPH.2023.307365. Epub 2023 Jul 20. Am J Public Health. 2023. PMID: 37471679 Free PMC article. No abstract available.
-
Association of Poor Sanitation With Growth Measurements Among Children in India.JAMA Netw Open. 2020 Apr 1;3(4):e202791. doi: 10.1001/jamanetworkopen.2020.2791. JAMA Netw Open. 2020. PMID: 32293682 Free PMC article.
-
A Qualitative Inquiry of Women's Perspective of Antenatal Education Services in Oman.SAGE Open Nurs. 2023 Mar 6;9:23779608231159336. doi: 10.1177/23779608231159336. eCollection 2023 Jan-Dec. SAGE Open Nurs. 2023. PMID: 36895708 Free PMC article.
References
-
- Haines MR. Inequality and infant and childhood mortality in the United States in the twentieth century. Explor Econ Hist. 2011;48(3):418‐428. 10.1016/j.eeh.2011.05.009. - DOI
-
- The World Bank . World Development Indicators | DataBank. DataBank. http://databank.worldbank.org/data/. Published 2015. Accessed July 7, 2017.
-
- Krieger N. Epidemiology and the People's Health. New York, NY: Oxford University Press; 2011.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
